The Patient A 64-year-old woman has called 911 because she has chest discomfort radiating to her left arm, palpitations, weakness, and a headache. She had a valve replacement (we do not know which valve) two weeks ago and has a healing incision over her sternum. She is found sitting in a chair, pale, cool, and diaphoretic. Her blood pressure is 94/palp. Her pulse rate is 196 bpm and weak. She is afebrile.
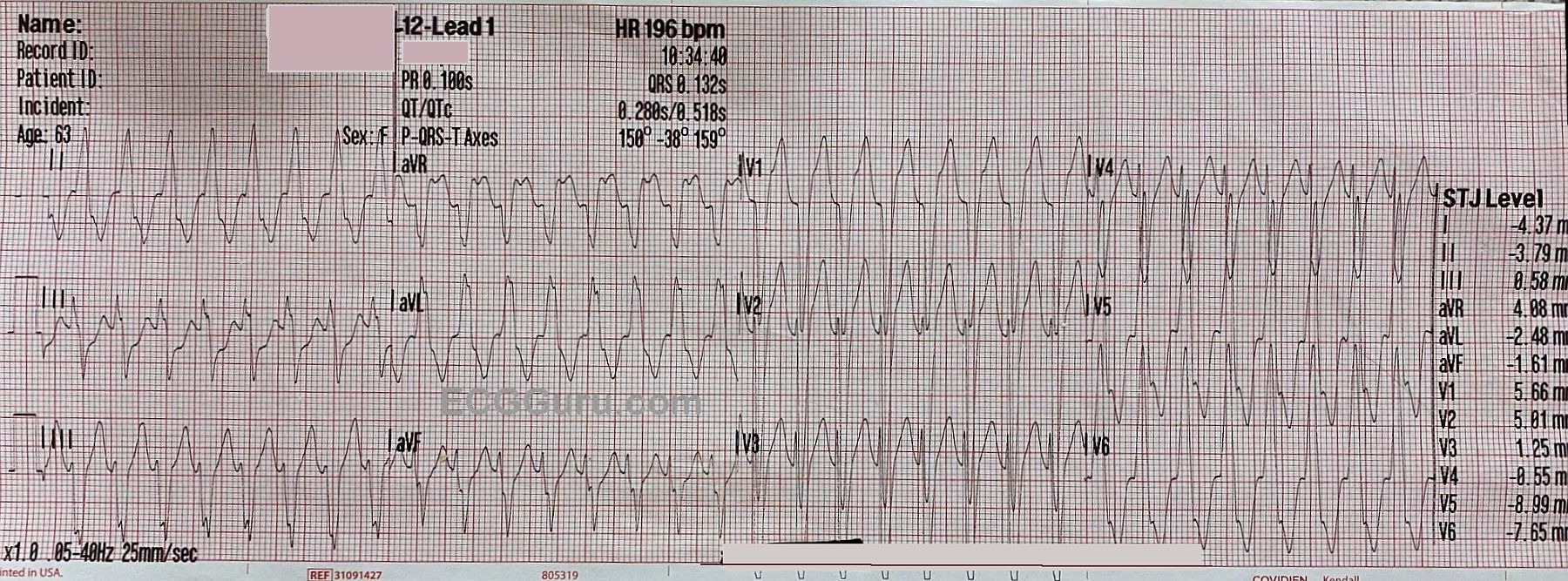
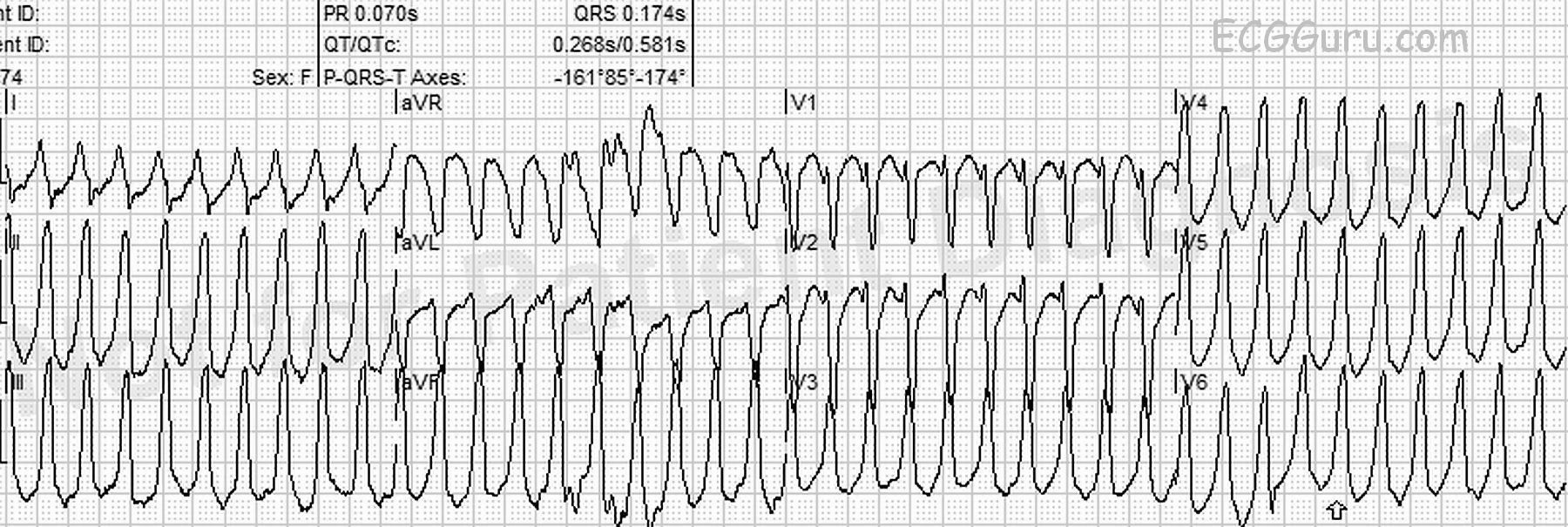
ECG #1 This ECG shows a wide-complex tachycardia at 196 bpm. The QRS complexes are .132 seconds in duration, per the ECG machine. The rate is too fast to appreciate whether there are P waves present. We did not see the onset of the tachycardia, but with a rate this fast and regular, it is most likely a reentrant rhythm, rather than sinus tachycardia. An abrupt onset of the rhythm would point to a diagnosis of a reentrant rhythm, either ventricular tachycardia (VT) or paroxysmal supraventricular tachycardia (PSVT).
There is an important rule in emergency medical care: a wide-complex tachycardia should be treated as VT until and unless it is proven to be something else. The most likely alternate interpretation is PSVT with aberrant conduction, which usually takes the form of left or right bundle branch block. Fortunately, the paramedics on this call have a protocol for treating WCT that includes electrical cardioversion for the unstable patient, and amiodarone for the stable patient. This protocol serves both possibilities, VT and PSVT, well. The patient’s perfusion status and BP made her borderline in this determination, but she was alert and oriented, so the paramedics opted for administering the amiodarone while they prepared to electrically cardiovert.