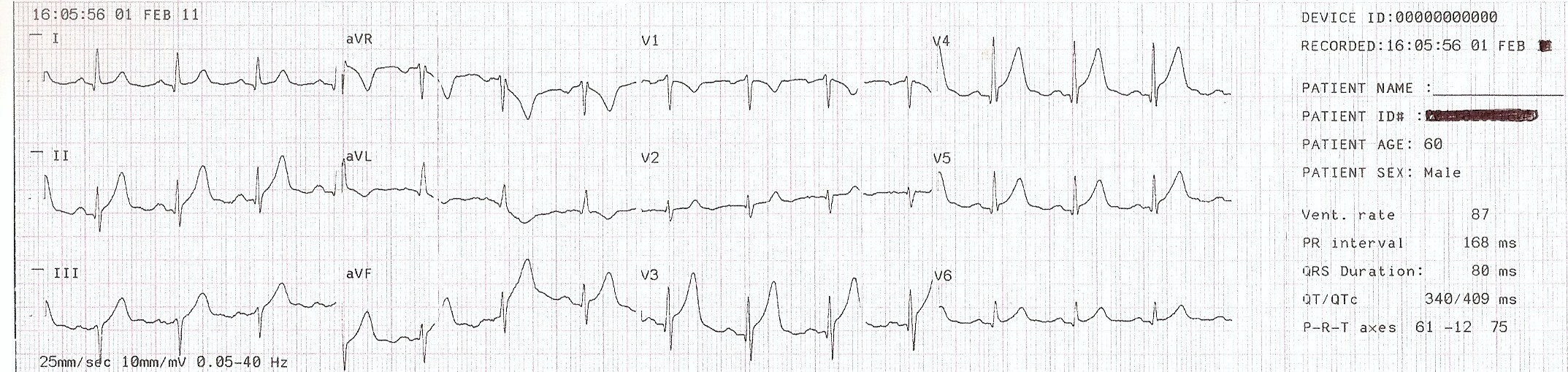
This ECG was taken from a 60 year old man who was complaining of severe substernal chest pain, radiating to his left arm and a non-productive cough. There was some initial discussion among the EMS crew about the possibility of the ECG showing a "benign early repolarization" pattern because of the concave upward ("smiling") ST segments. They also considered a diagnosis of pericarditis, because the ST segments seem widespread. The baseline artifact makes it difficult to evaluate for PR segment depression or Spodick's Sign.
The patient's age (60 years) and troubling symptoms (chest pain radiating to the left arm) ruled out BEP for the paramedics. The ST segment elevations are pretty widespread - Leads V3, V4, V5, V6, I and II all show some STE. There are also "hyperacute" T waves in the leads with STE. There are ST abnormalities ranging from flattening of the shape to depression, but the bottom line is this patient is a 60-year-old man with substernal chest pain radiating down his left arm!
The patient was treated in the ambulance with chest pain protocols, and was transferred to a hospital with an interventional cath lab. The patient was conculusively diagnosed with an acute M.I. and underwent angioplasty.
This is a good ECG to demonstrate subtle changes when, combined with patient presentation, can help us diagnose a coronary event. It helps us emphasize that not all STEMIs will have dome-shaped, "tombstone" ST segments, and that patient symptoms, history, and age are important to consider.