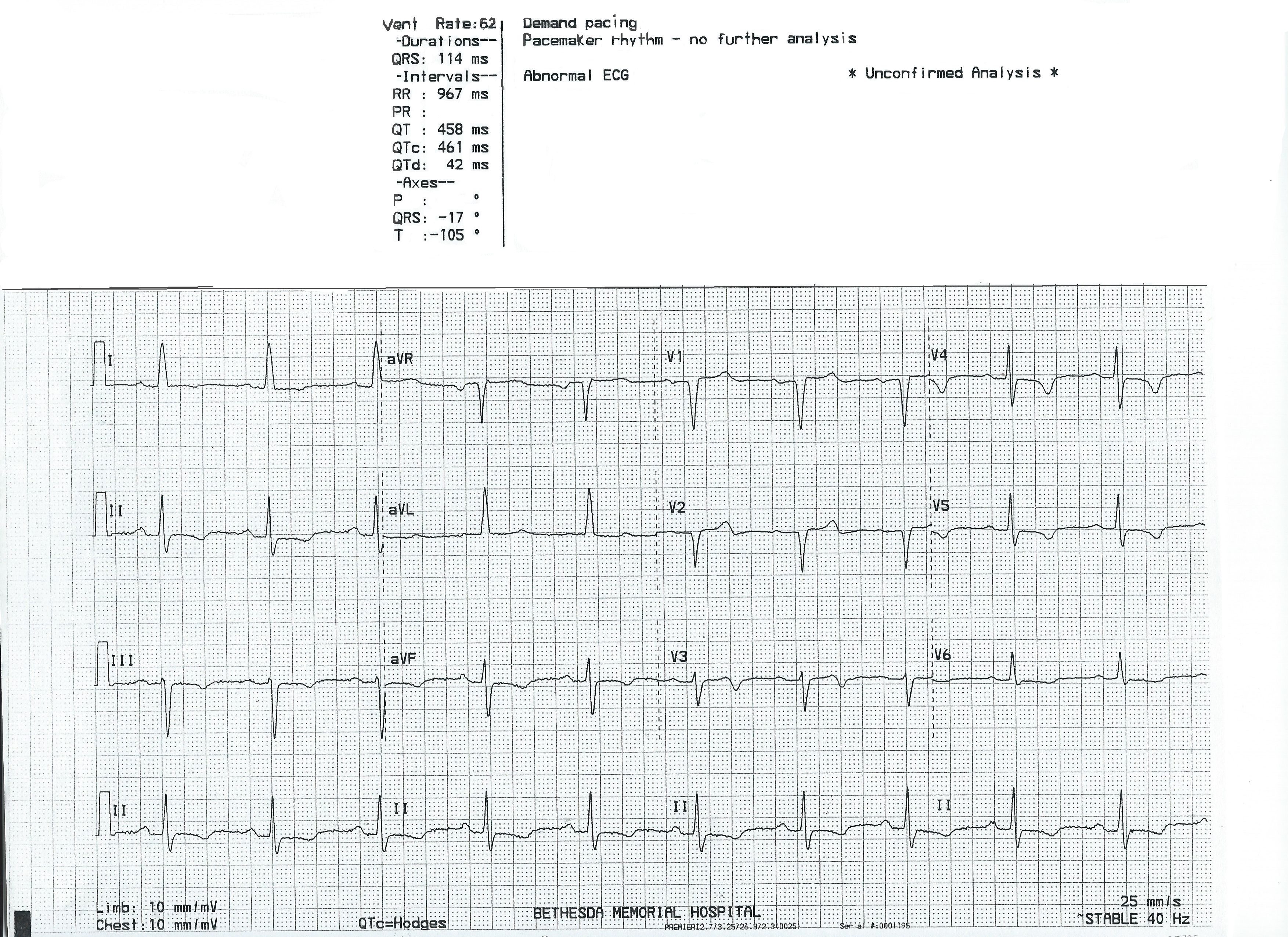
This ECG is presented as an example of INCORRECT MACHINE INTERPRETATION. While there are many abnormalities in this ECG, it does not represent a paced rhythm. While there are exceptions, most paced rhythms represent either AV sequential pacing, right ventricular pacing, or bi-ventricular pacing.
RECOGNITION OF A PACED RHYTHM
Recognizing a paced rhythm can be difficult in some cases. Because pacemakers now have so many programmable features, there is a wide variety of ECG changes associated with them. Pacer “spikes” can be difficult to see in all leads. Finding evidence of the device on the patient’s chest or via patient history is a big help in reminding us to scrutinize the ECG for paced rhythm.
An AV sequential pacemaker or a right ventricular pacemaker will pace the ventricles via the right ventricle. This produces a WIDE QRS and a leftward axis, often causing Leads II, III, and aVF to be negative and aVL and aVR to be positive. Along with the wide QRS, we will see DISCORDANT ST CHANGES. That is, there will be ST depression and T wave inversion in leads with positive QRS complexes and ST elevation and upright T waves in leads with negative QRS complexes.
Bi-ventricular pacing can be a little more complicated to recognize, as the QRS can be narrow, with signs of fusion between the wave produced by the LV electrode and the RV electrode.
The frontal plane axis is usually far right – aVR will be positive. Lead I will be negative.
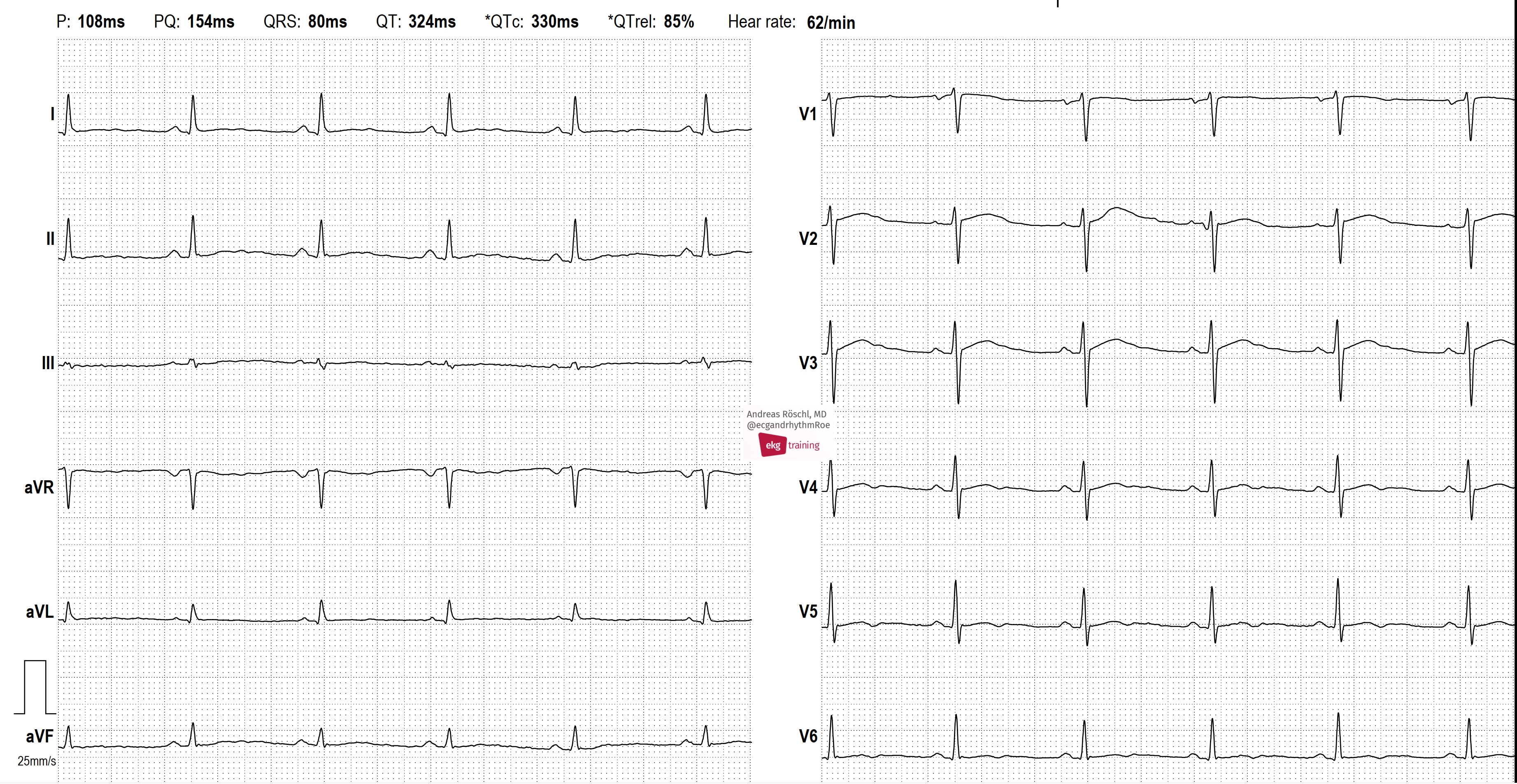
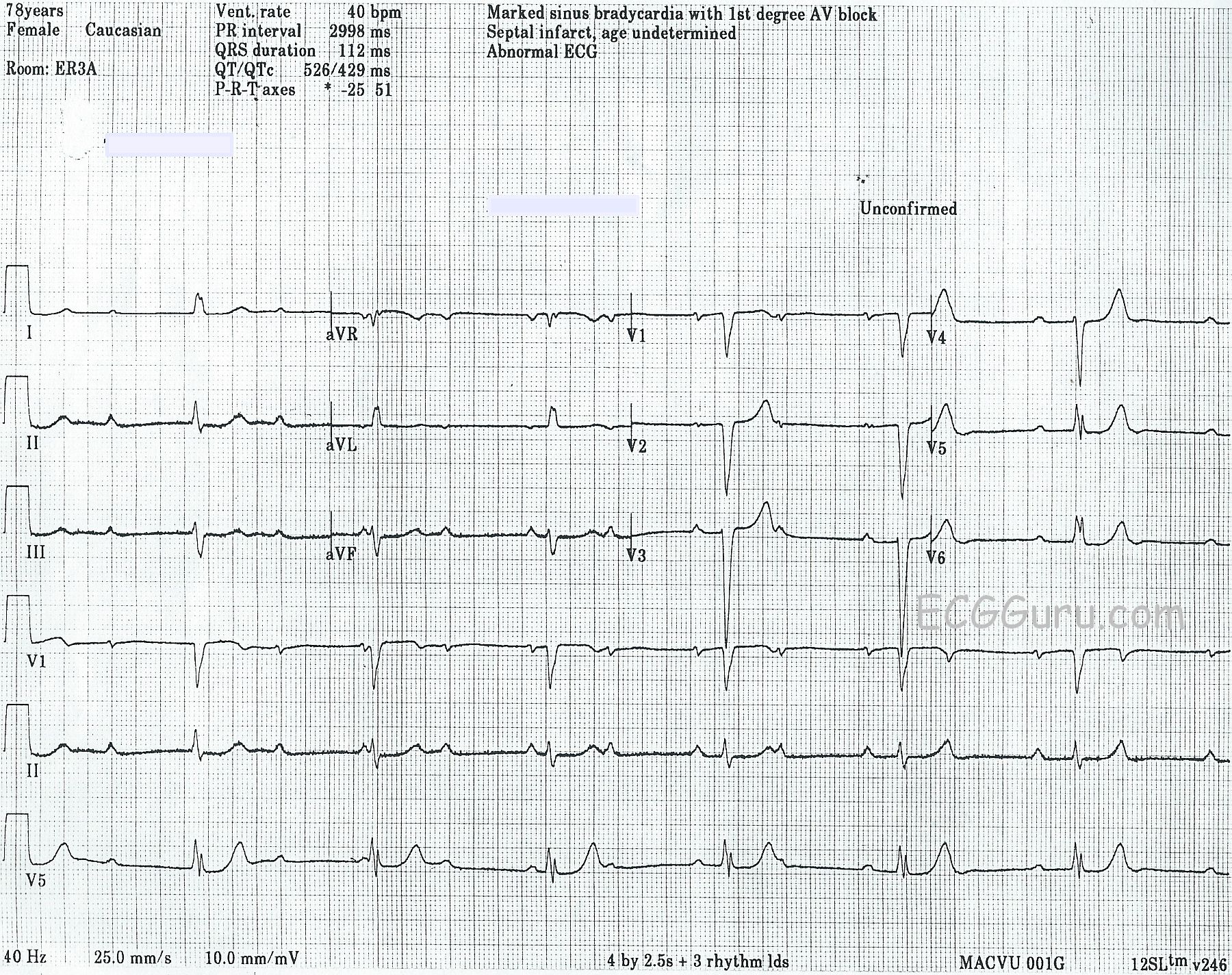
The machine is wrong: there is no indication of a pacemaker, and P waves are present, even though they are not noted in the "PR Interval" or "P Axis".
SO, THIS IS NOT A PACED RHYTHM – WHAT IS IT?