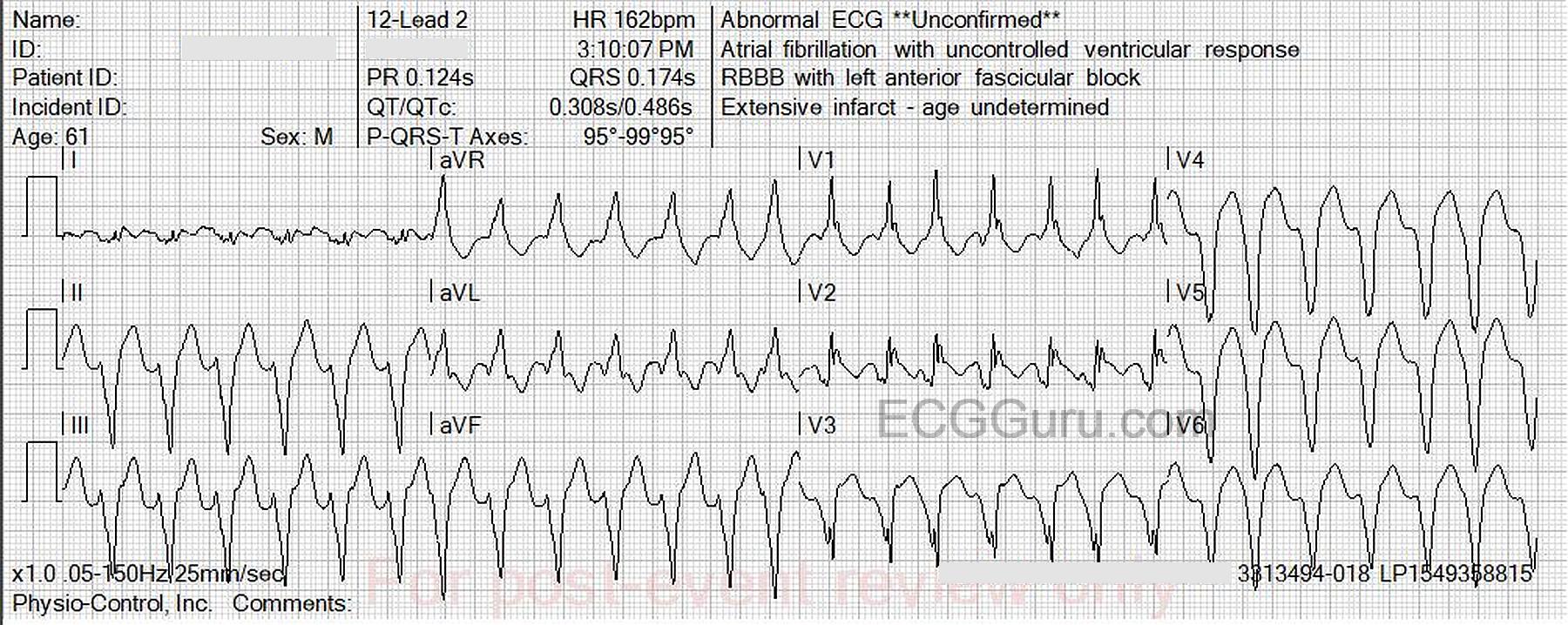
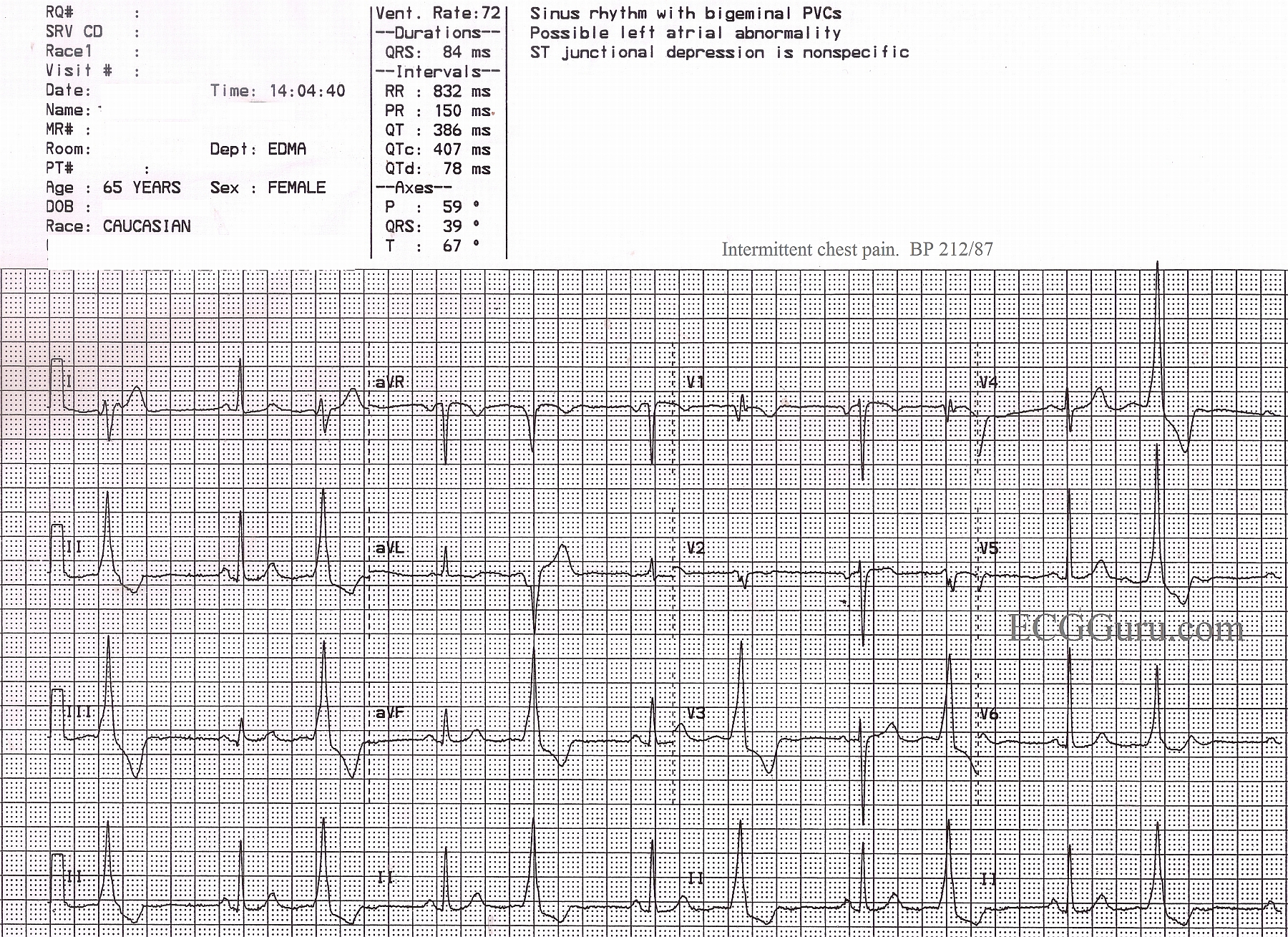
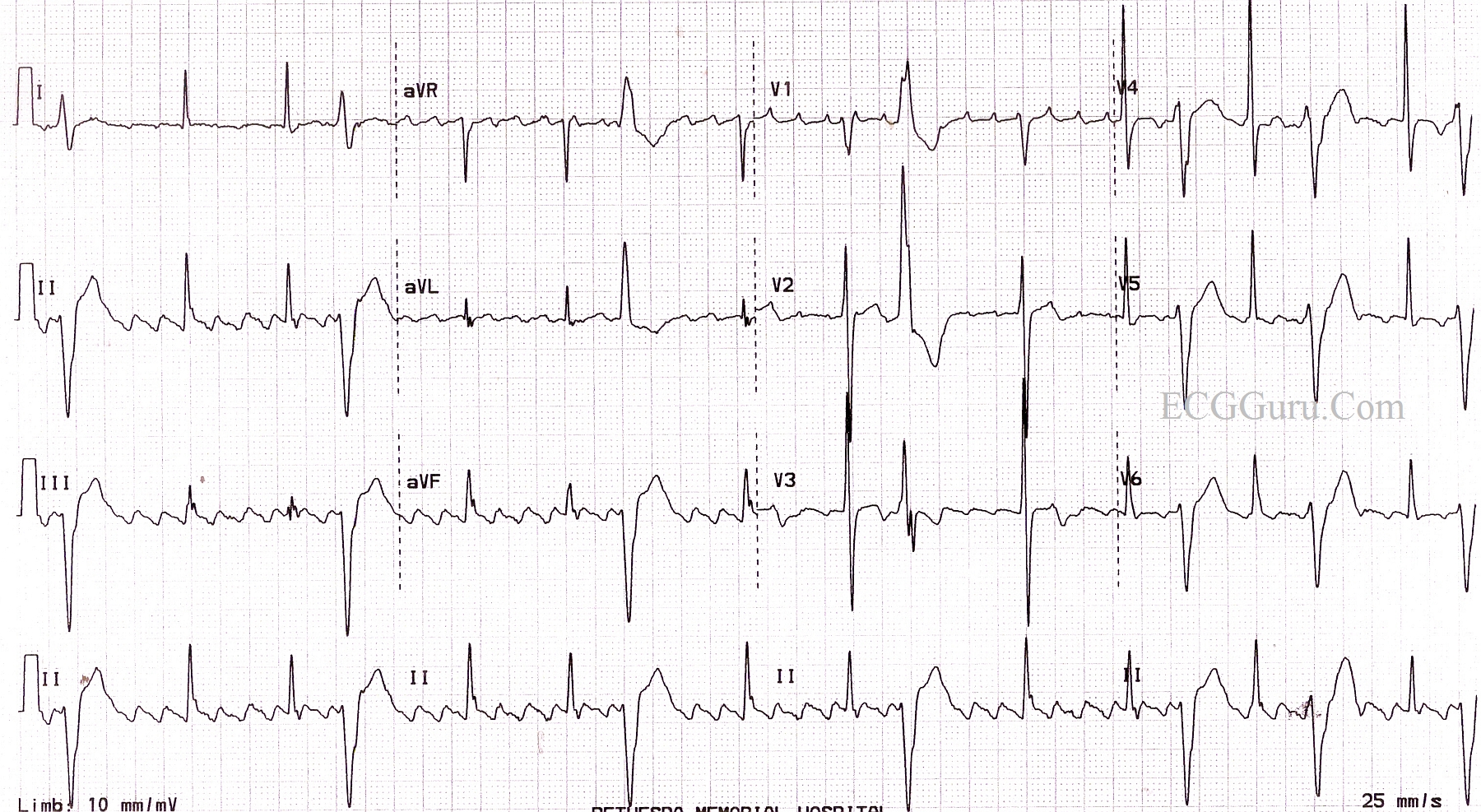
Unbelievably, this inferolateral ST elevation M.I. was missed by the treating paramedics in the field. An elderly woman stepped off a curb and was hit by a very slow-moving car. She fell and sustained a Colle's fracture of the right wrist. While the paramedics assessed her, she complained of chest pain, prompting them to perform a 12-Lead ECG. The machine's interpretation called attention to the inferior and lateral walls' injury pattern, but the paramedics did not believe it, because "she was a trauma patient". They ran three ECGs, and still did not agree with the machine.
The patient was transported to a hospital without an interventional cath lab, and she was forced to endure a one-hour wait to be transferred to an appropriate hospital.
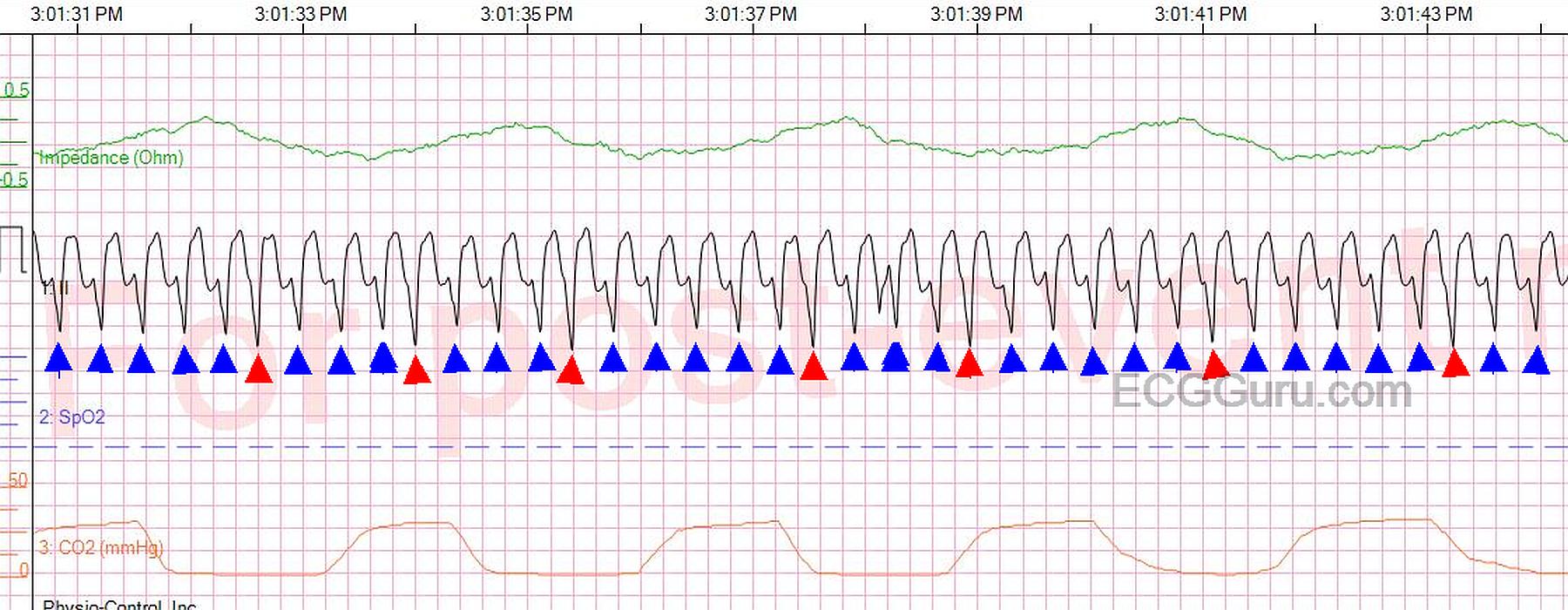
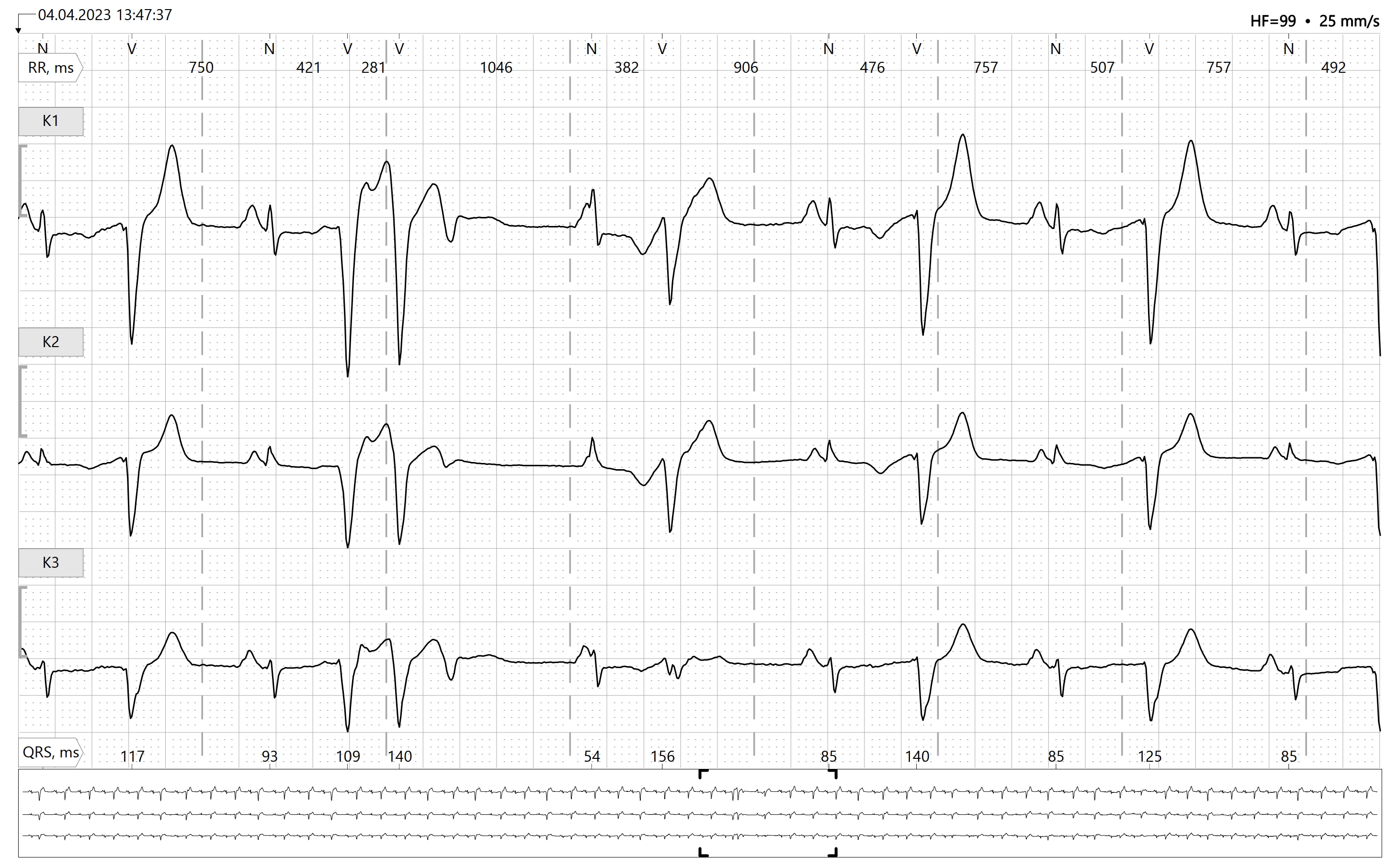
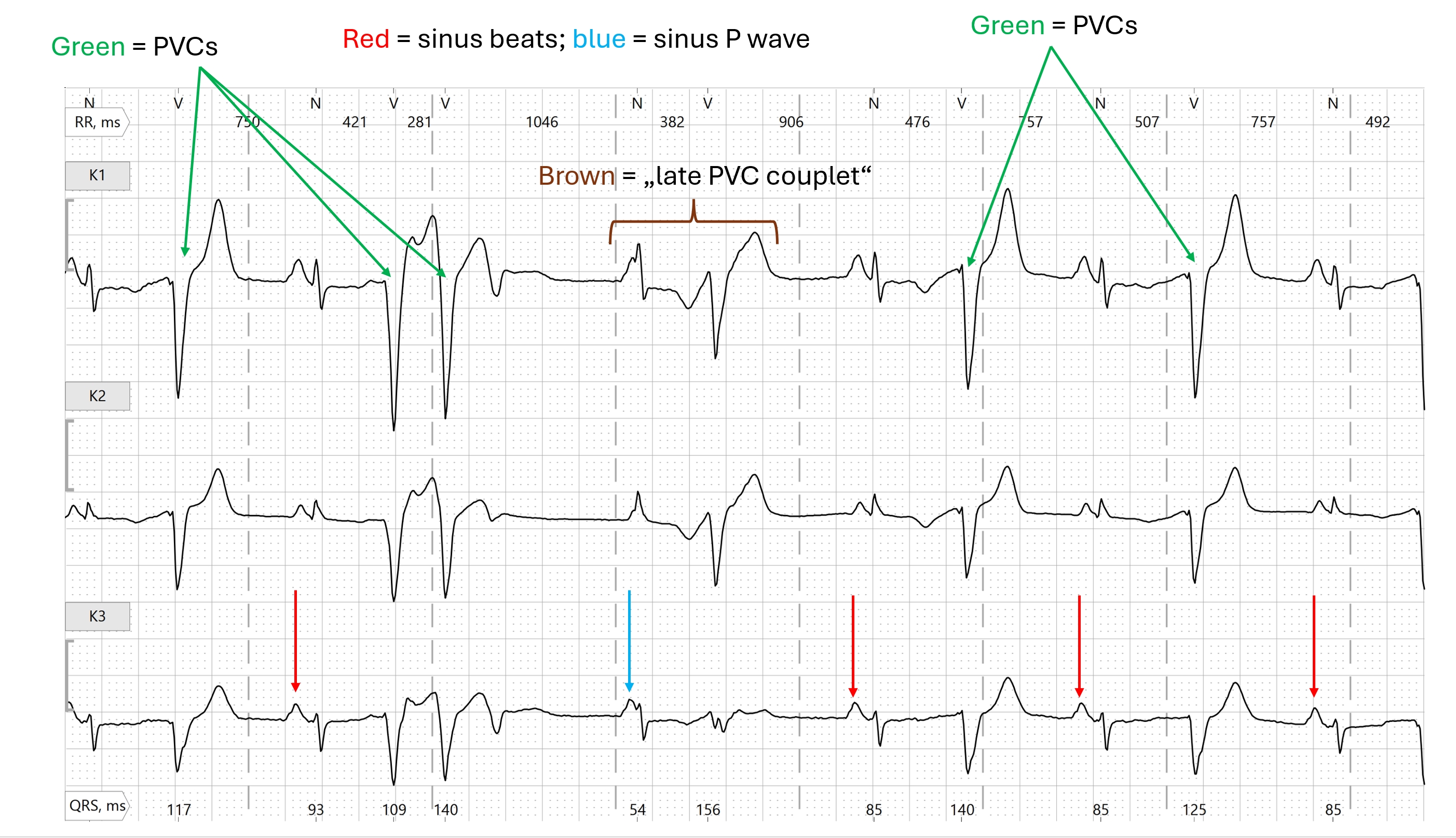
This is a great ECG for a discussion with your students about "distractors". The call came in as a trauma, so that, in itself, was a distractor. The rescuers saw what they expected to see. The angulated fracture distracted them - putting them into full trauma assessment mode. Then, the frequent and coupled PVCs also distracted them, possibly making it more difficult for them to evaluate the ST segments in the normal beats. Interestingly, the second and third ECGs did not have PVCs, and the ST elevation was even more clear.
PVCs which are repeating themselves in groups of two, three, or more are sinister in a chest pain patient, and may indicate LV dysfunction. They could possibly result in ventricular tachycardia, which would be disasterous for this patient.