The patient: This ECG is taken from a 55-year-old man whose wife called 911 because he had a syncopal episode. When the paramedics arrived, he was conscious and alert, and denied any symptoms. He gave a history of "cardiac", diabetes, and opiate abuse. We do not know the nature of his cardiac history or his medications.
It is difficult to pinpoint a definite diagnosis with this lack of information and a clearly abnormal ECG. We will limit our discussion to listing the abnormalities seen:
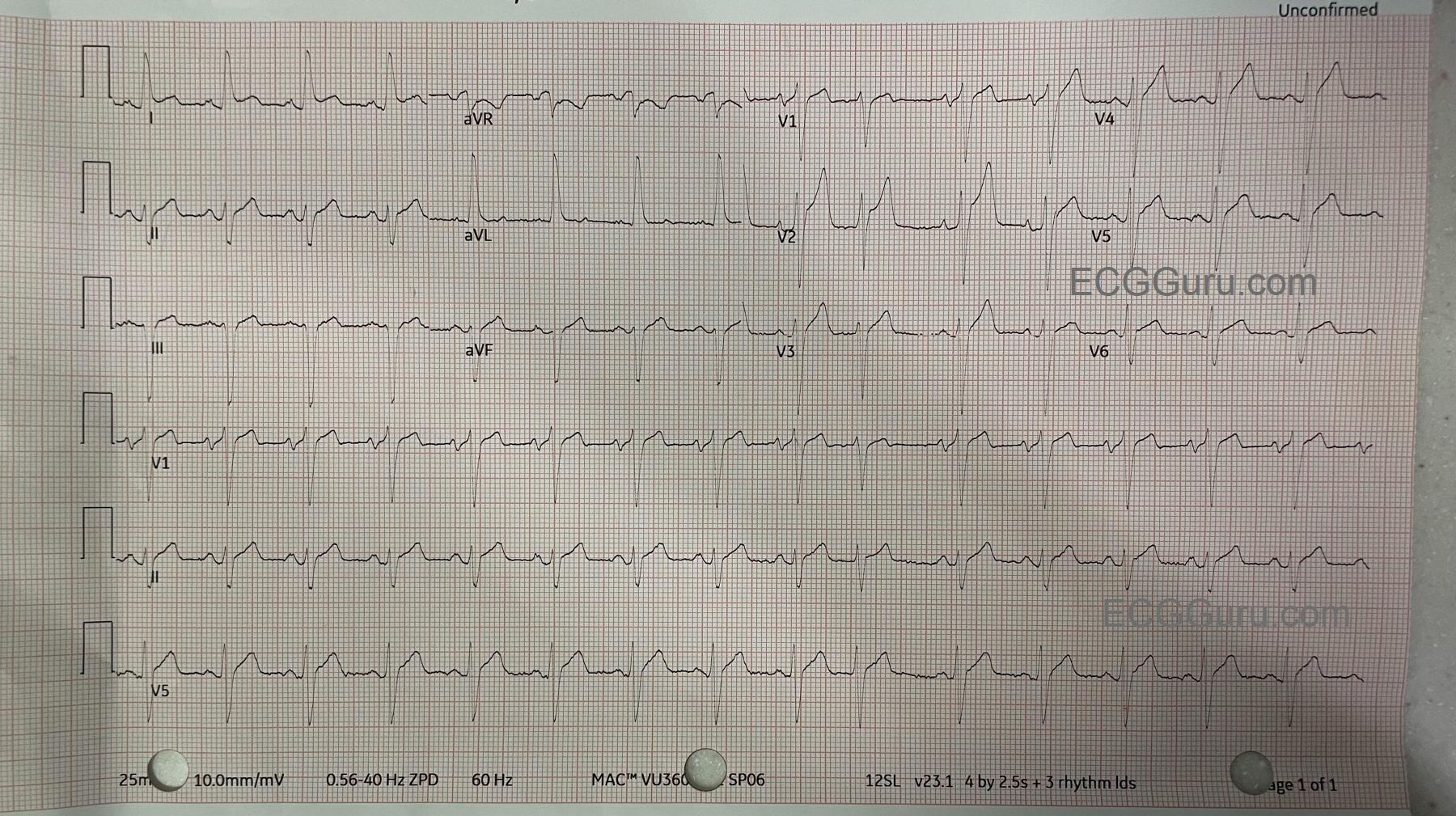
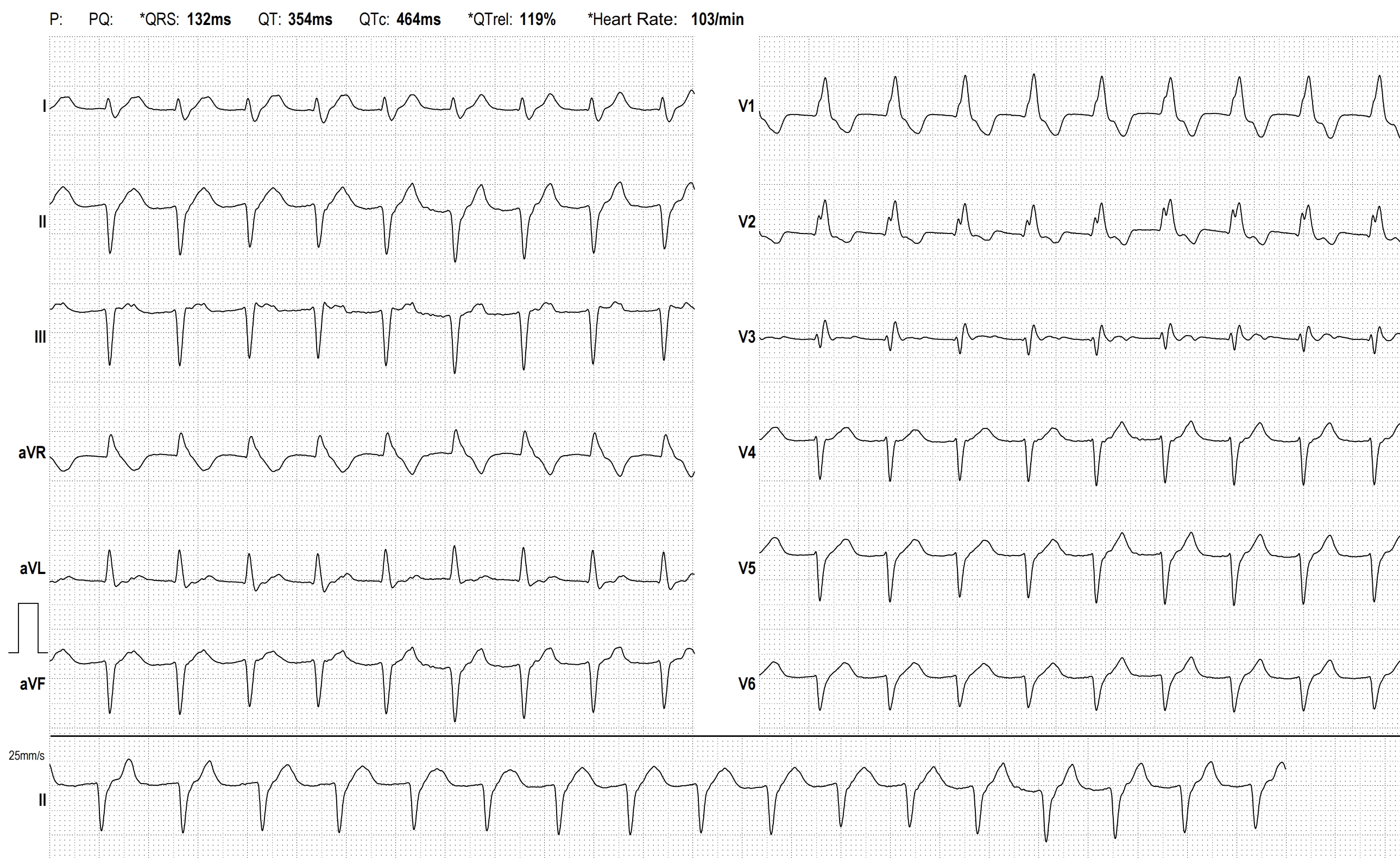
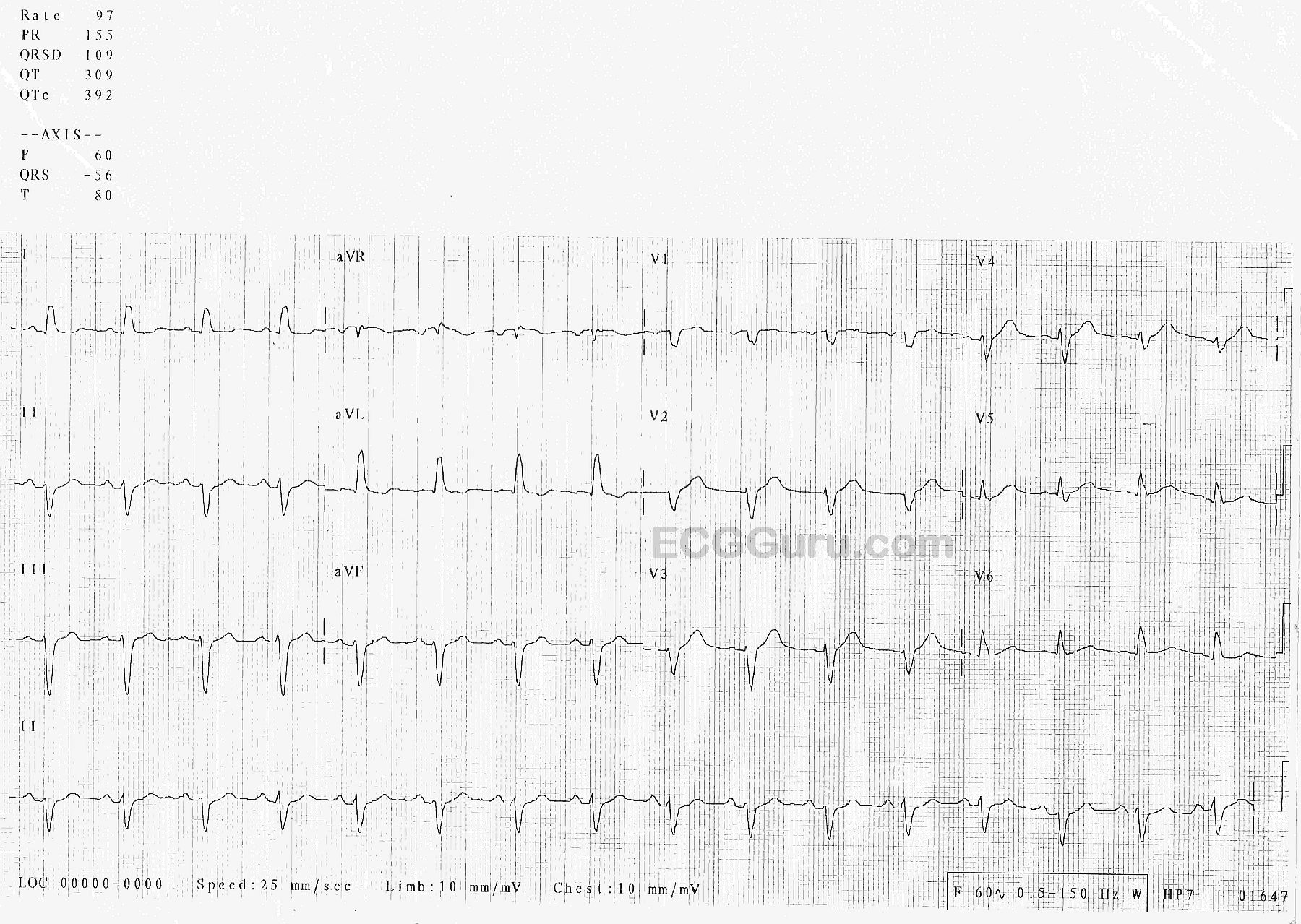
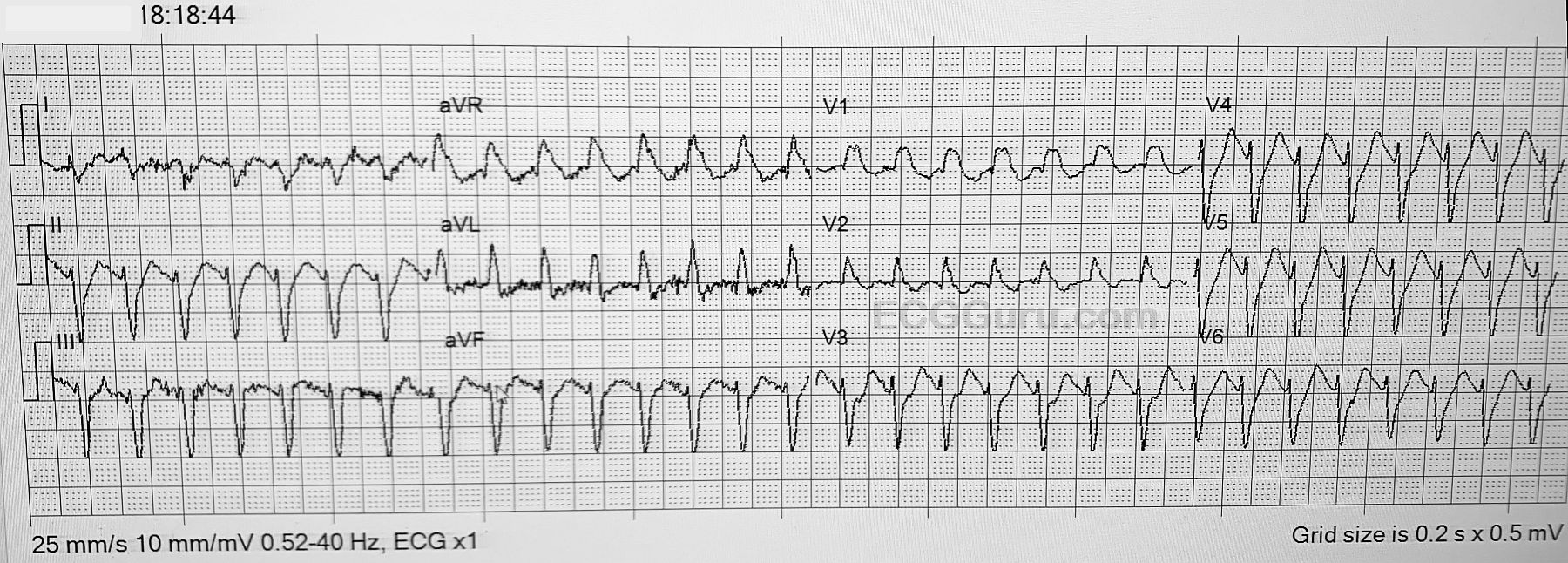
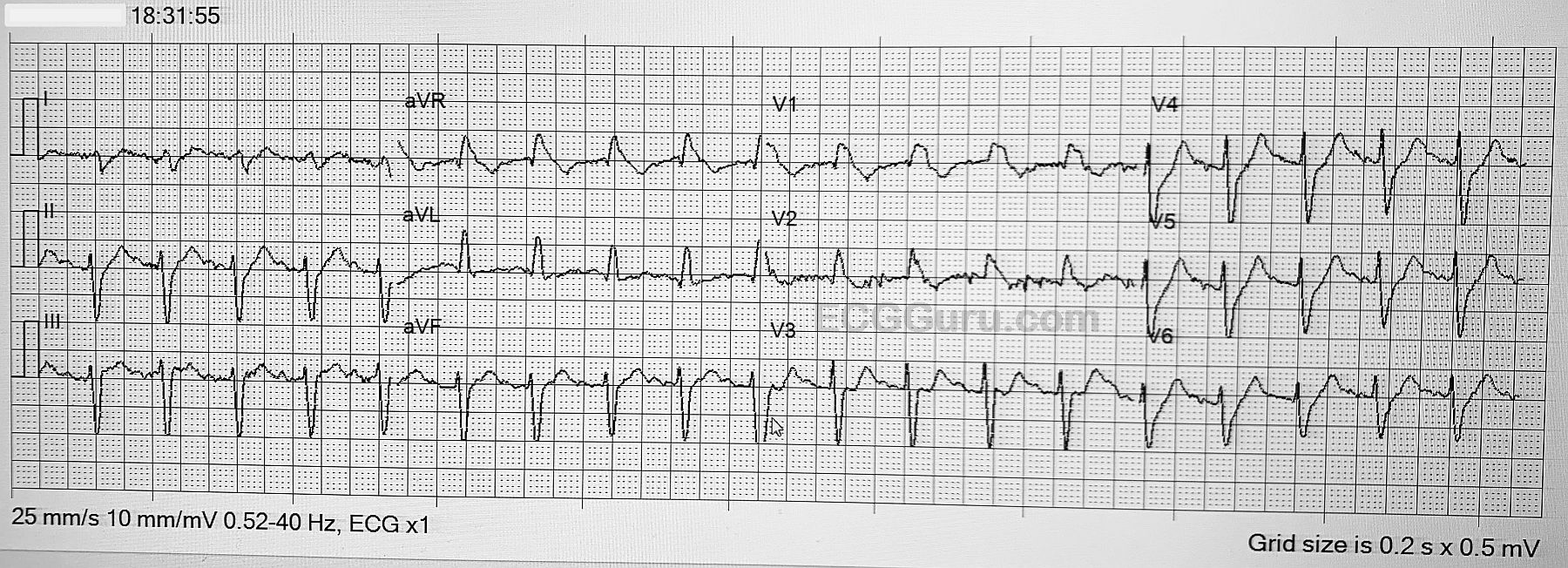
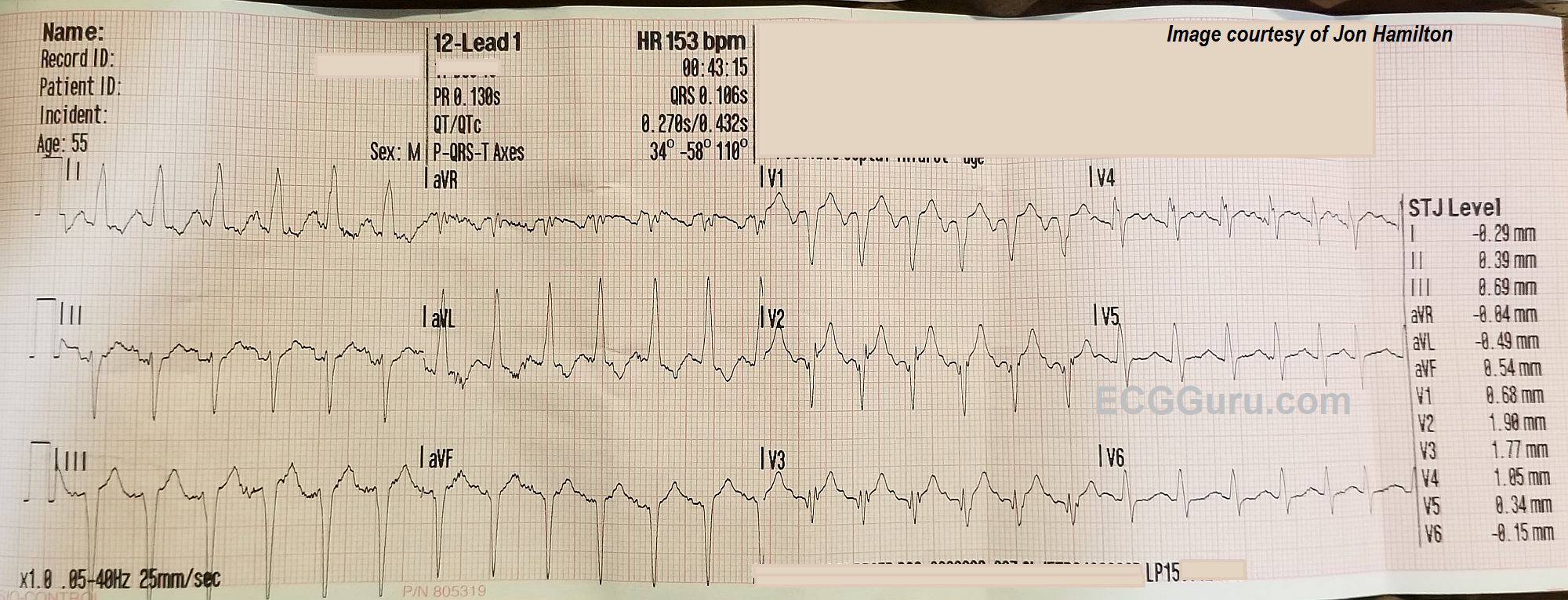
The ECG rhythm: There is a fast, regular rhythm that is supraventricular in origin (there are P waves). When a supraventricular rhythm has a rate of about 150 per minute, we should ALWAYS consider ATRIAL FLUTTER WITH 2:1 CONDUCTION. Atrial flutter produces P waves (flutter waves) at approximately 250-350 per minute. The normal AV node is able to conduct half of these, at a rate of about 150 per minute. Atrial flutter with 2:1 conduction is the most common presentation of new-onset atrial flutter. It is often missed by people who expect to see several flutter waves in a row, producing the "sawtooth pattern". That being said, atrial flutter is usually discernable in at least a few leads if it is present. We do not see any signs of flutter waves in this ECG.
That leaves us with a differential diagnosis of sinus tachycardia vs. one of the regular supraventricular tachycardias like reentrant tachycardias or atrial tachycardia. Sinus tachycardia can be recognized by several features. If we are fortunate enough to witness the onset or offset of the fast rhythm, will will recognize sinus tachycardia by a "warm up" or gradual speeding up of the rate, and a "cool down", or gradual slowing. On the other hand, SVTs often have abrupt onset and offset. Sinus tachycardia often has a very obvious cause, such as hypovolemia, fever, pain, anxiety, vigorous exercise, or hypoxia. Sinus tachycardia usually has a distinct, upright P wave in Lead II, and a clearly-seen, often negative, P wave in Lead V1. This ECG does not show the onset of the tachycardia, and is not long enough to evaluate for rate changes. Lead II appears to have upright P waves on the downslope of the previous T waves. V1 has deeply negative P waves, and V4 has the most clearly-seen P waves. Without being positive, this looks more like sinus tachycardia than a reentrant tachycardia. It would help to know more about the patient's condition.