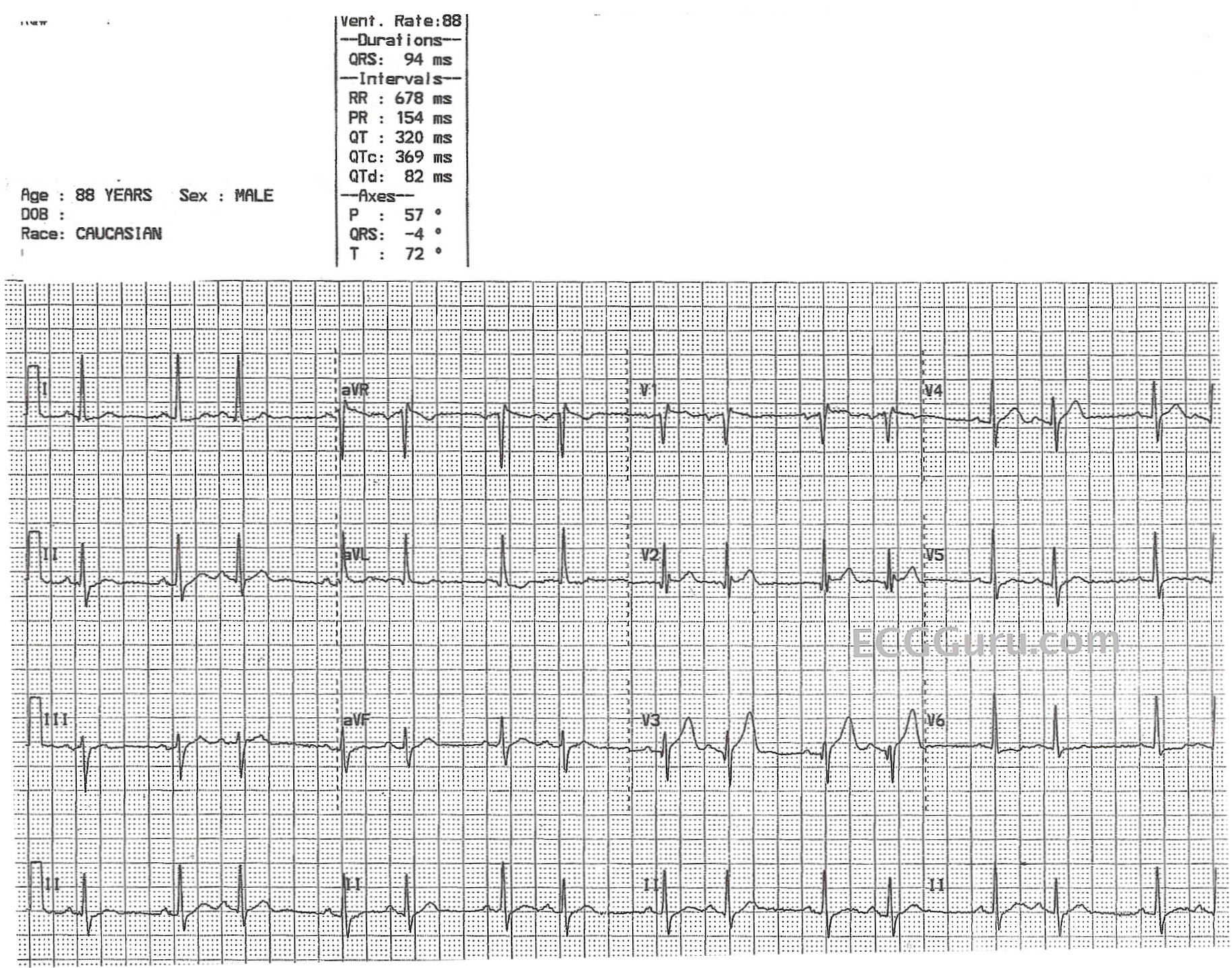
This strip offers something interesting for both your basic-level students and for your more advanced students. First, it is a good example of sinus rhythm with a premature beat. The PR interval was measured by the machine at .21 sec (218 ms). The premature beat is supraventricular - that is, it is not a PVC. Because of the slightly long PRI in this strip, it's P wave COULD be buried in the preceding T wave. That would make this a premature atrial contraction (PAC).
For discussion with your more advanced students, the P wave could, instead, be retrograde, and occurring during the QRS or slightly after it. That would make the premature beat junctional, or an atrial echo beat. The origin of the premature beat is mostly academic - there is likely no clinical need to determine the origin.
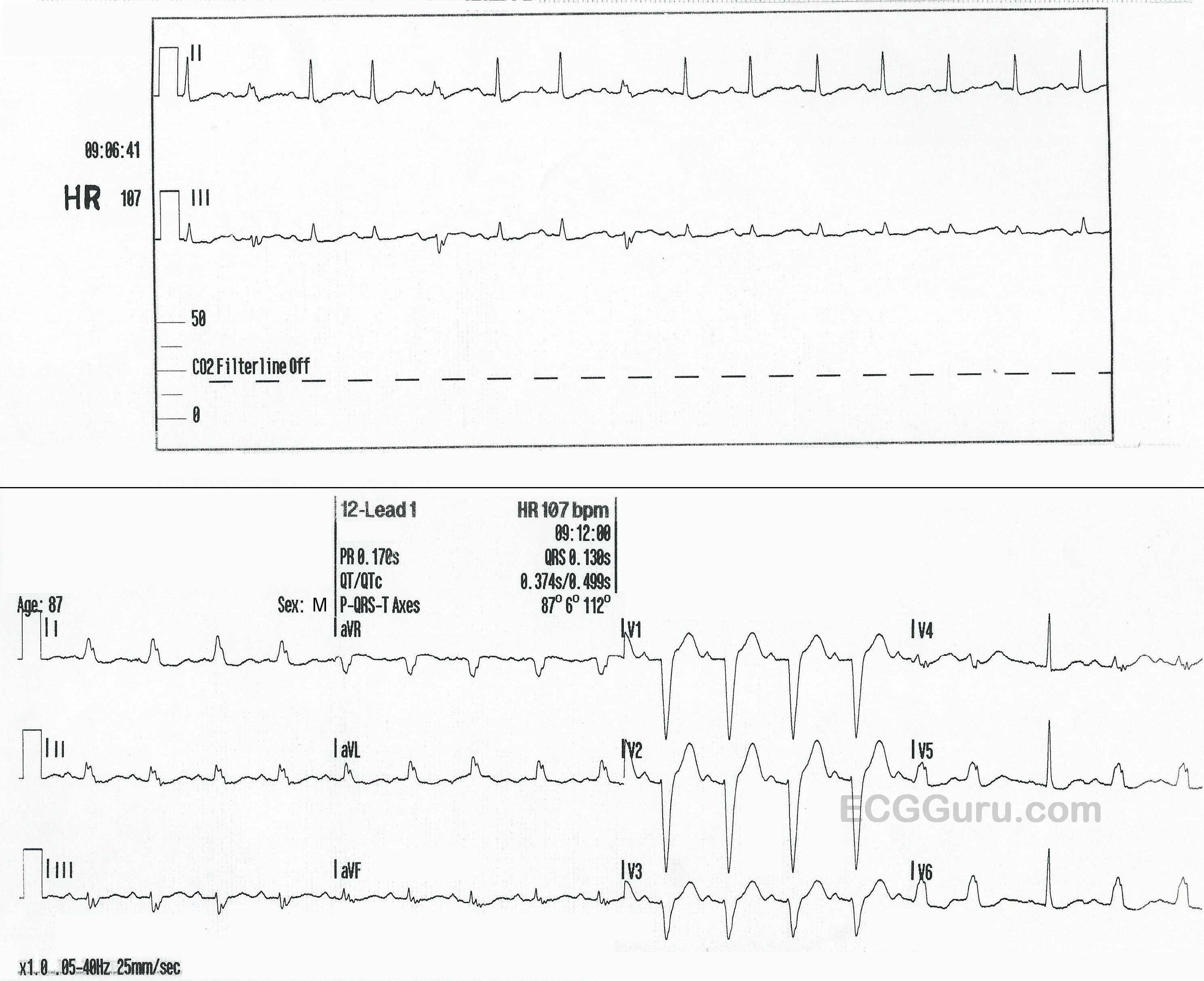
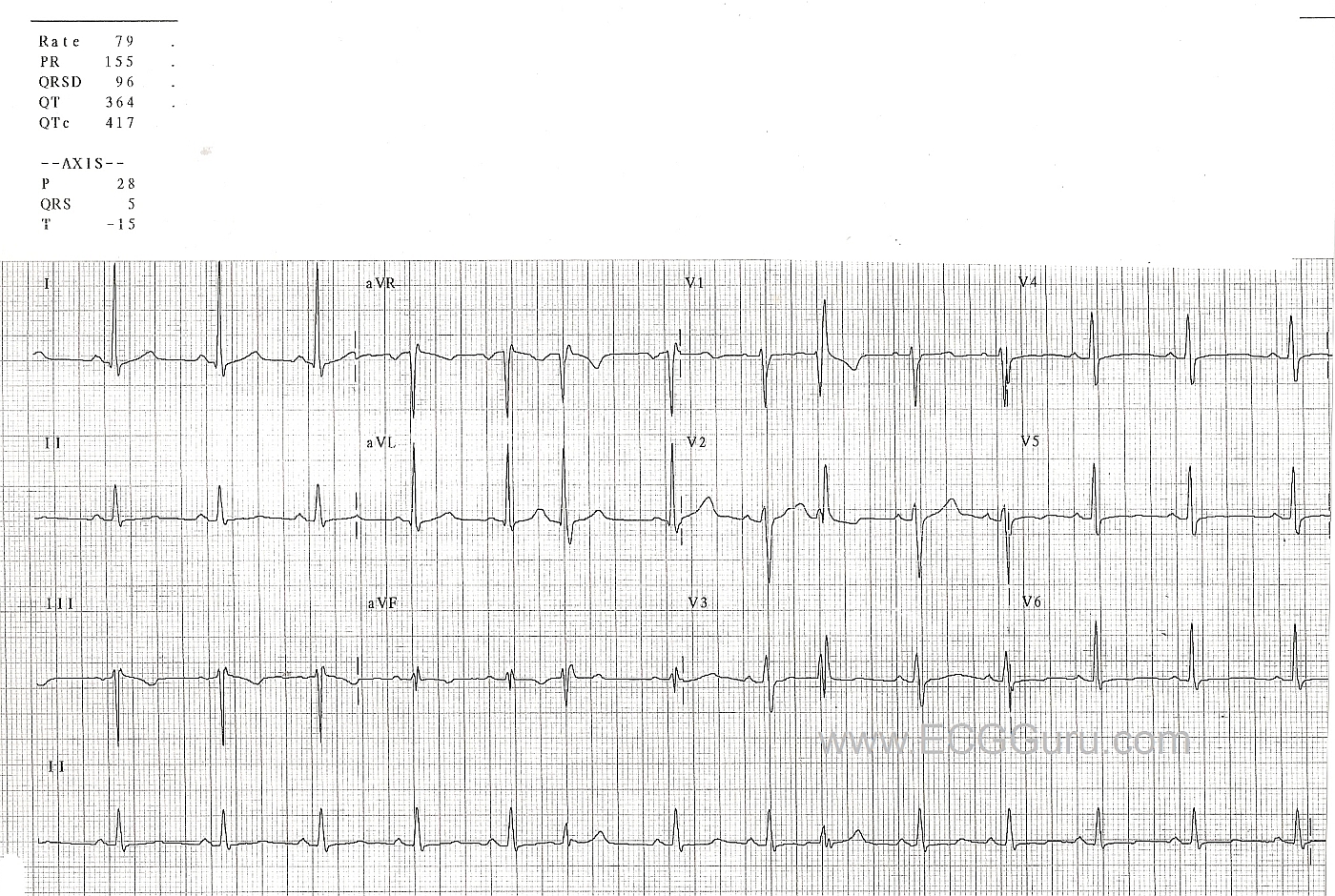
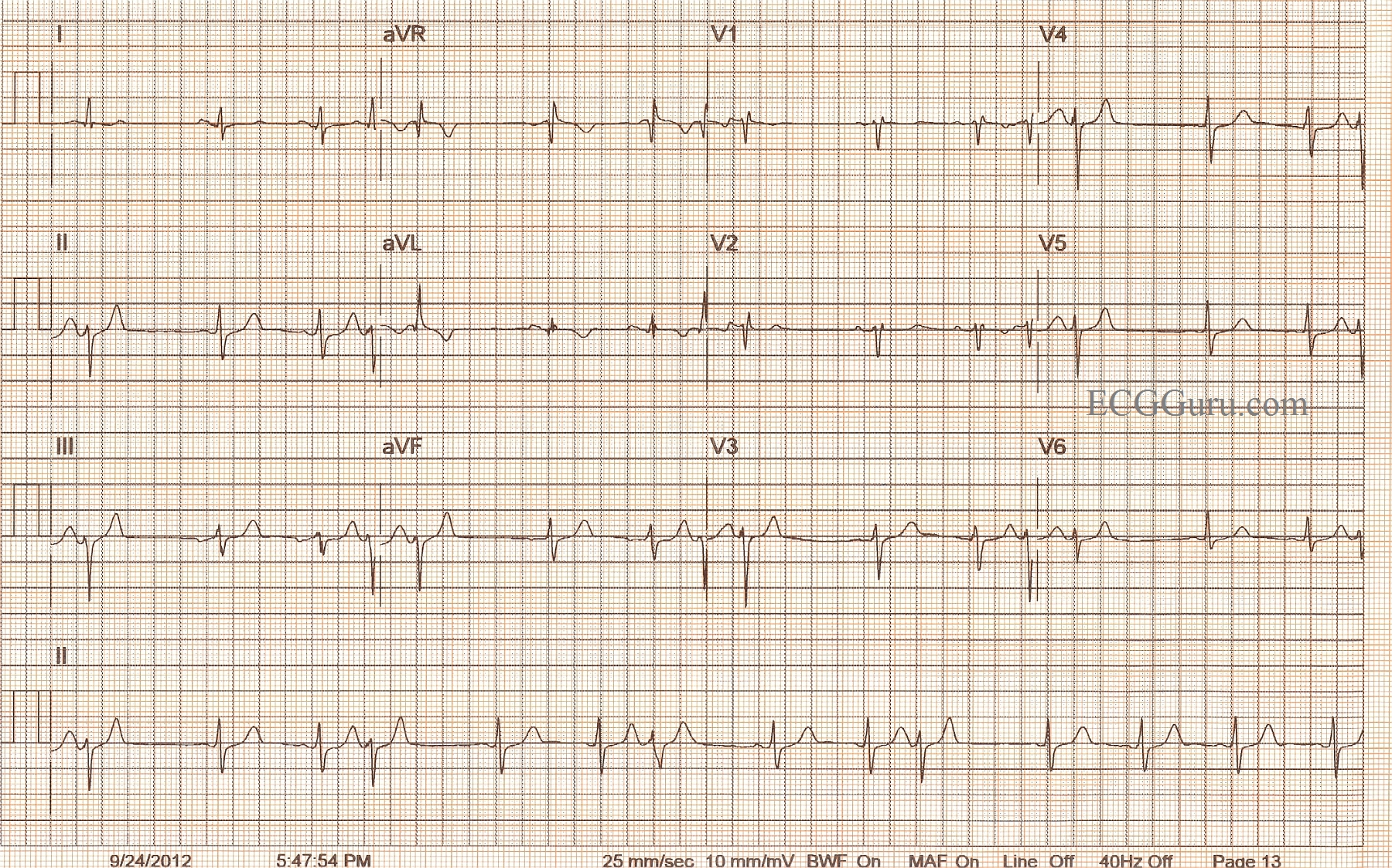
In looking for clues as to the origin of the premature beat, we would scrutinize the premature beats for "hidden" P waves. Upright and before the premature beat would indicate a PAC. Negative P waves before, during, or after the premature QRS would indicate PJCs. In this strip, the T waves just before the premature beats are slightly deeper than the other T waves. This could indicate atrial "echo", or reciprocal beats, which requires the presence of dual junctional pathways, in which the impulse turns around, reenters the atria, and causes a new beat. It can be helpful to look at multiple leads (the more the better) in your search for P waves. For a look at this patient's 12-lead ECG, go to this link.
The P wave of a premature beat often penetrates the SA node and "resets" it, causing the next normal beat to occur after a "normal" R-to-R interval from the premature beat. This fact can help us find "hidden" P waves, as well.
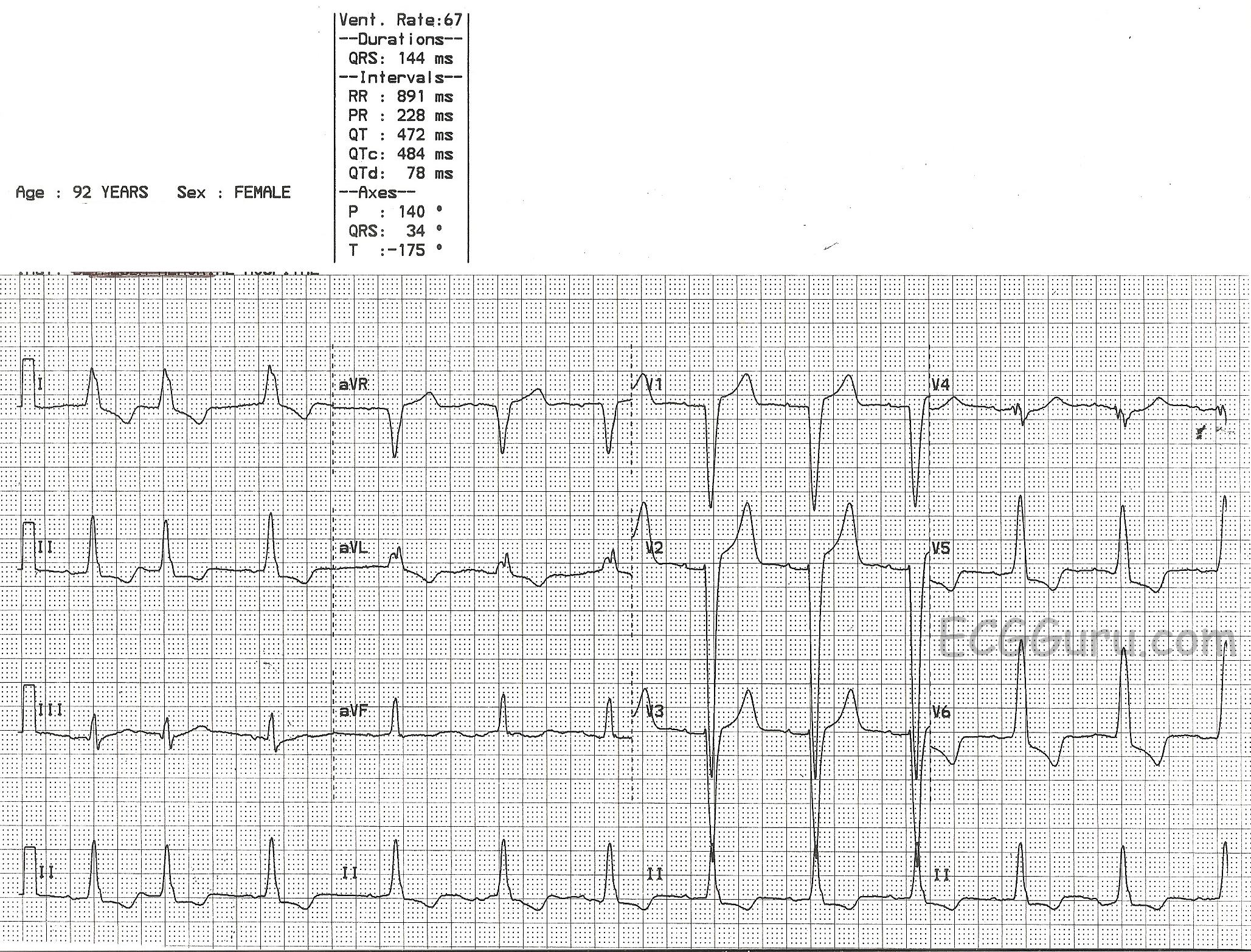
Another interesting feature of this strip for your students who are interpreting 12-Lead ECGs, is that this ECG shows the criteria for left ventricular hypertrophy. See the link above for the 12-lead and discussion.