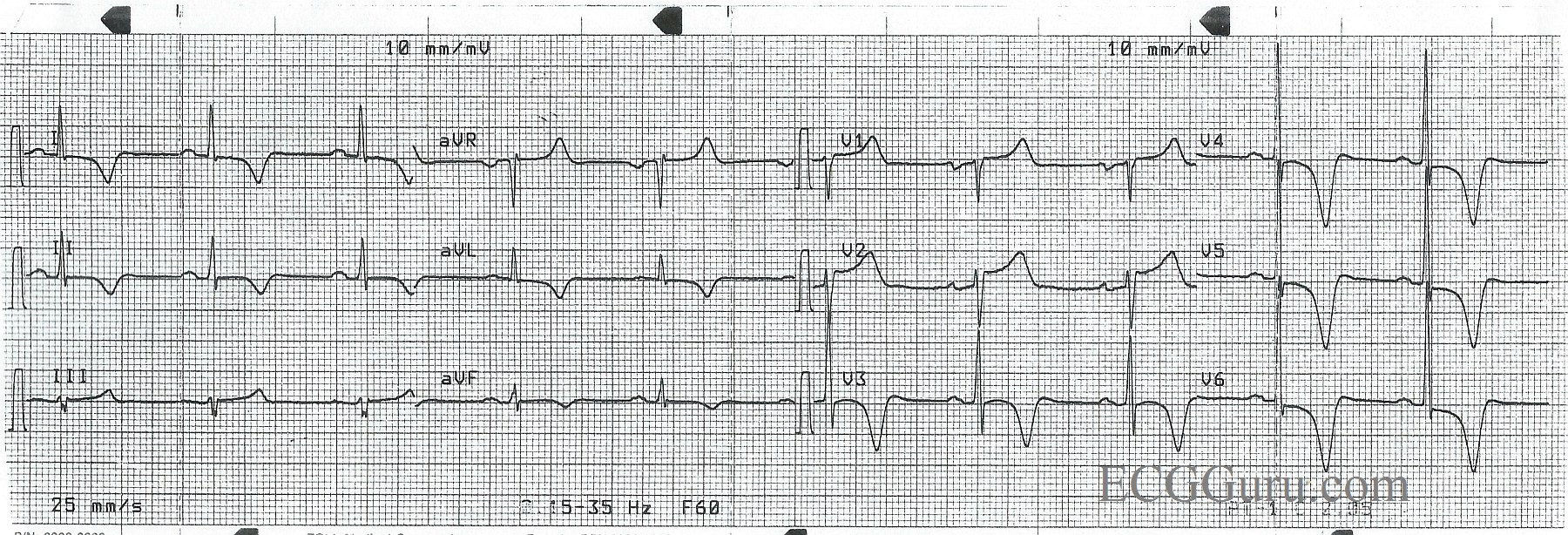
This ECG is from a 50-year-old man with chest pain. Unfortunately, we don’t have any other clinical information. This tracing is a good example of widespread, symmetrical inverted T waves. Inverted T waves are present in Leads I, aVL, II, and V3 through V6. (The anterior-lateral leads). There are ST segment elevations in Leads V1 and V2.
Many conditions can cause inverted T waves, and bedside assessment is necessary to make a certain diagnosis. Some T wave inversions are benign, such as in persistent juvenile T wave pattern. Some can be due to life-threatening problems like pulmonary embolism, CNS injury, and cardiac ischemia. T wave inversions can be secondary to conditions like left ventricular hypertrophy, left bundle branch block, and ventricular rhythms. When T waves are deep and symmetrical as they are here, they may be a sign of acute coronary syndrome, or cardiac ischemia. Since we know this patient had chest pain, and there is some ST elevation, this should be considered as a cause for his T wave changes.
In addition to the dramatic T waves, he also has P waves suggestive of “P mitrale”, or left atrial enlargement. The P waves in Lead II are wide (about 10 or 11 ms) and just over 1 mv tall. This is “borderline” for most LAE criteria. The P waves in Lead V1 are biphasic, with the second portion negatively deflected and over 1 mv deep. Acute myocardial infarction can cause left ventricular dysfunction, which can cause backup pressure to the left atrium.
Inverted T waves, like all ST and T wave changes, should always be assessed in the context of the patient presentation, history, and previous ECGs, if available.
References: Consultantlive.com, Dr. Ken Grauer