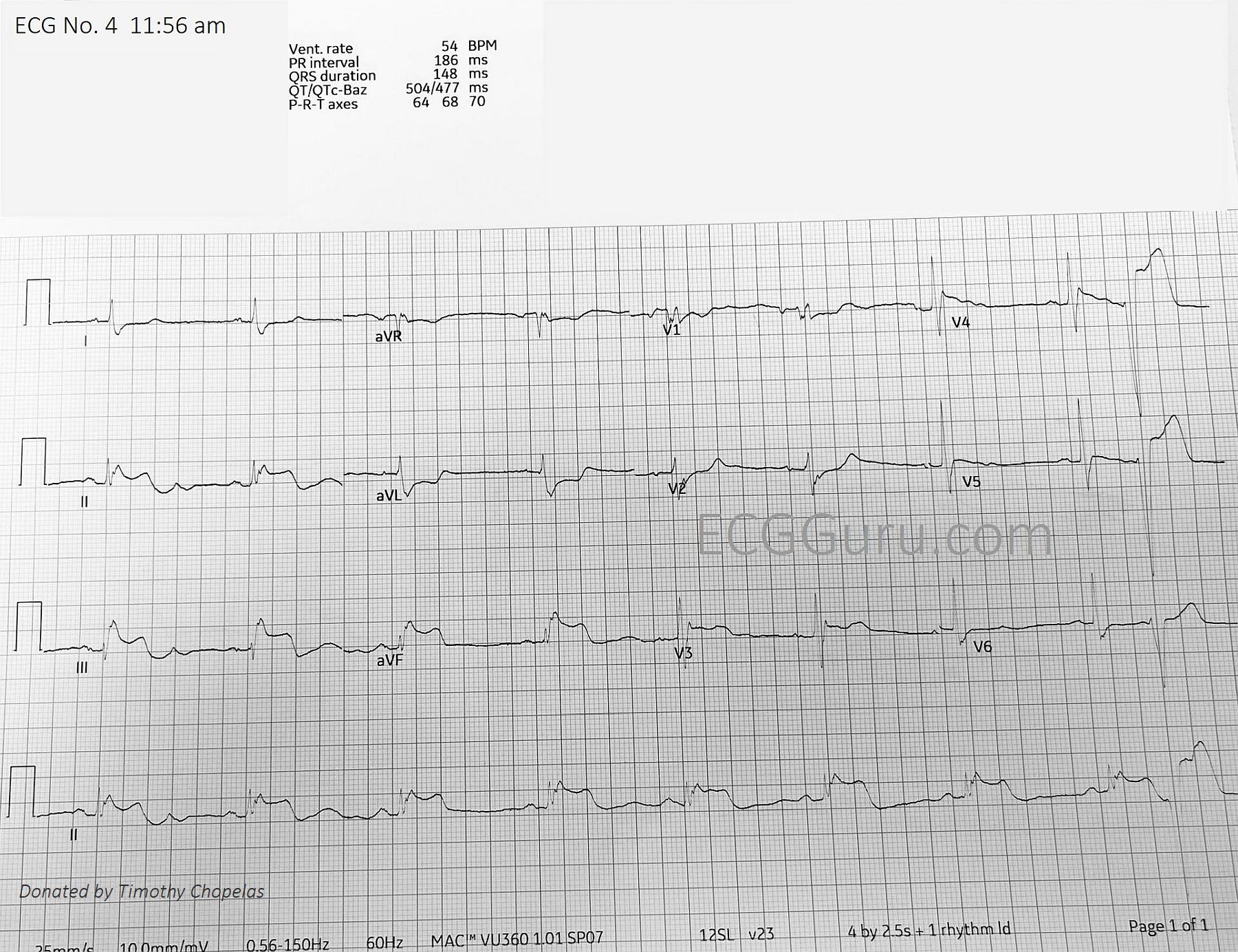
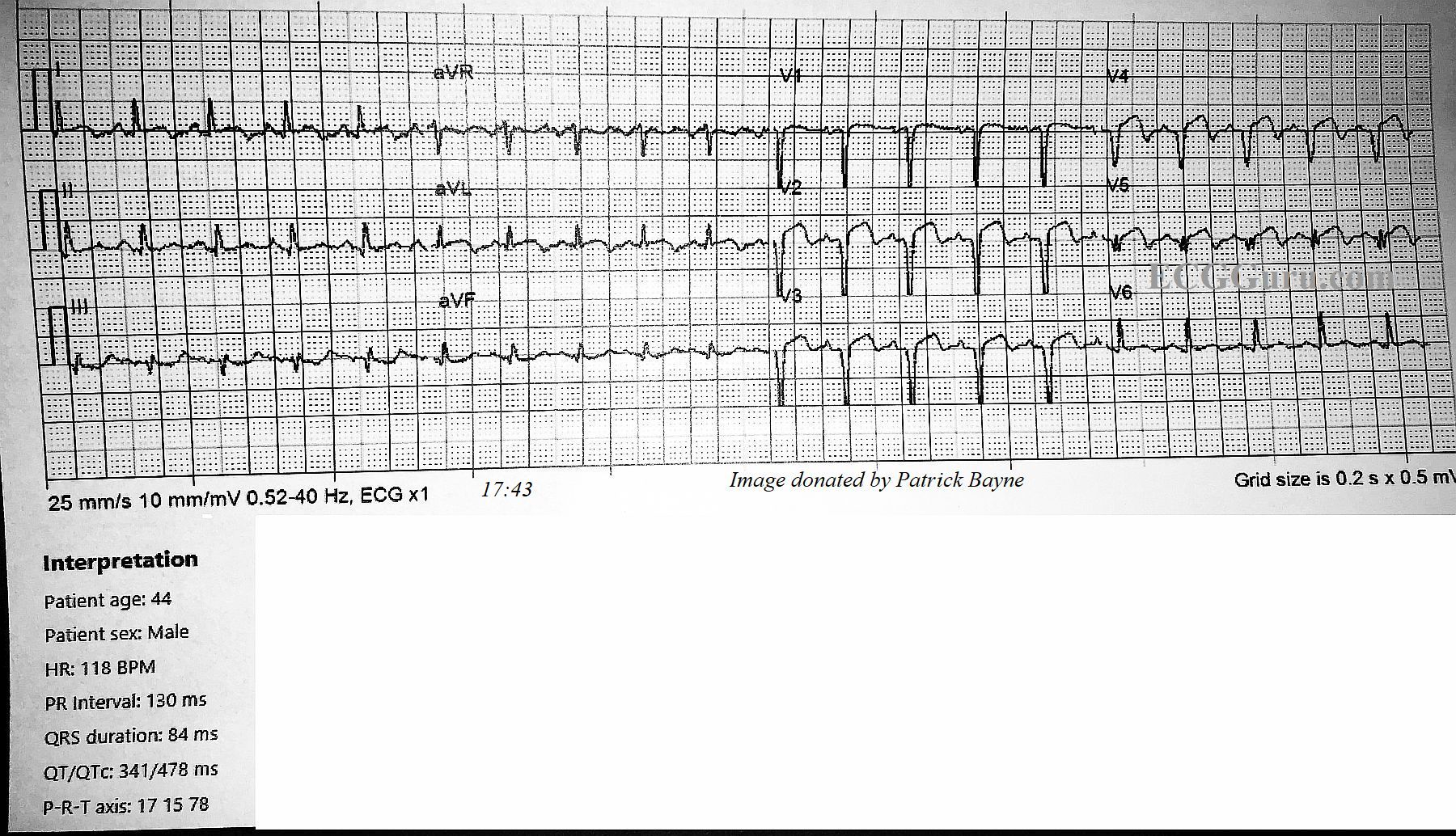
This ECG was taken from a 78-year-old man who was experiencing chest pressure in the morning, after having left shoulder pain since the night before. He has a history of hypertension and hypercholesterolemia, and has an implanted pacemaker.
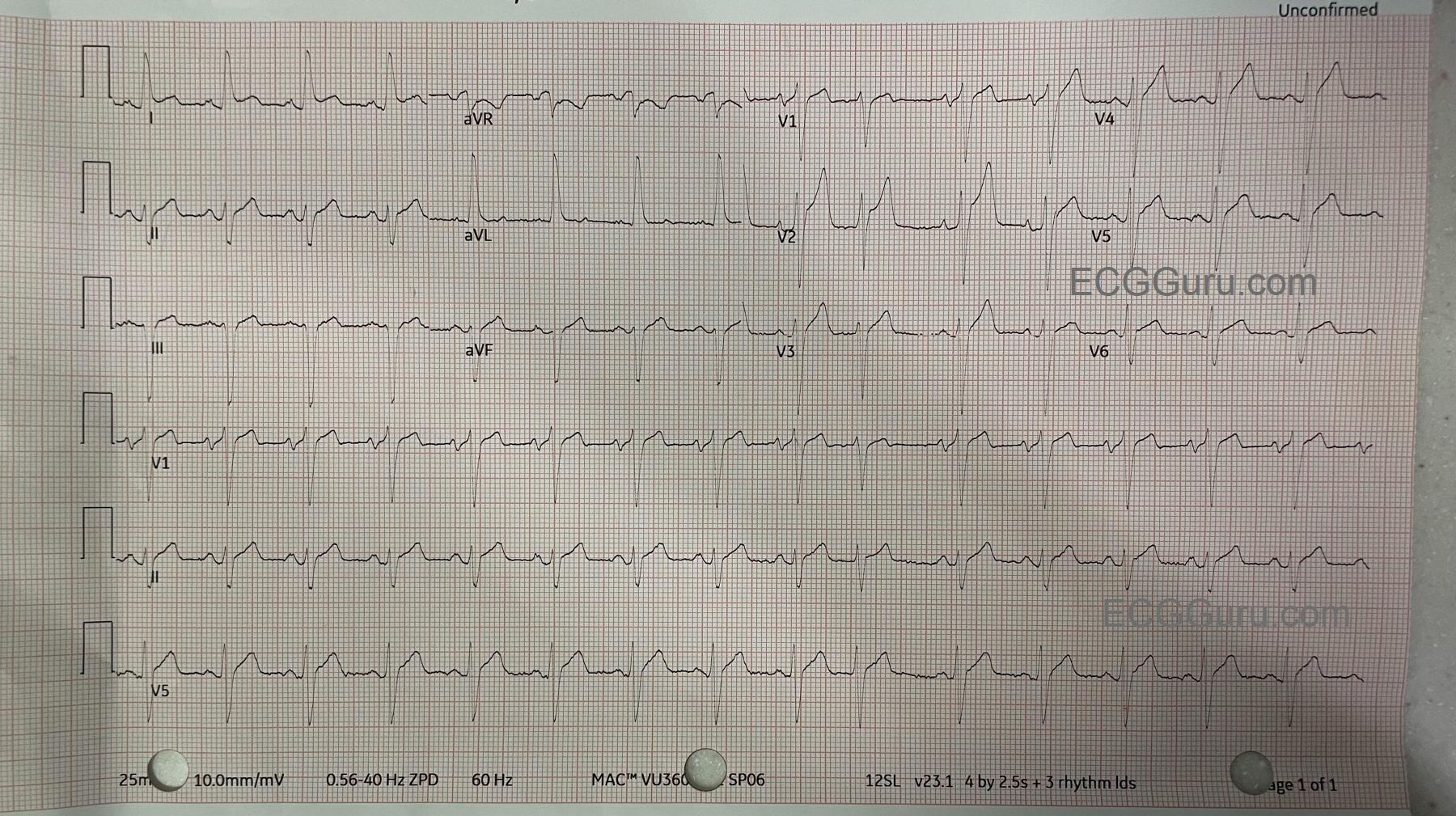
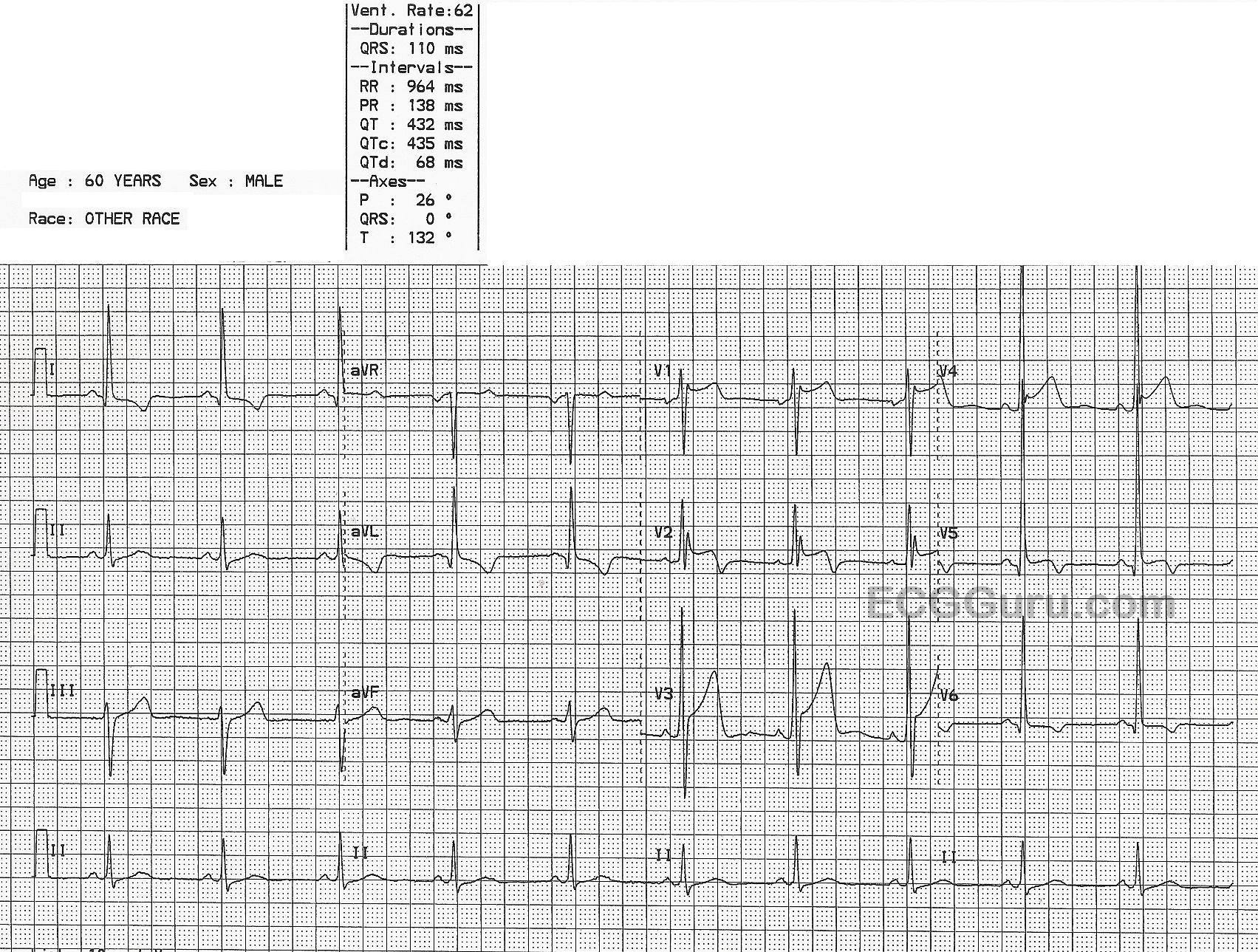
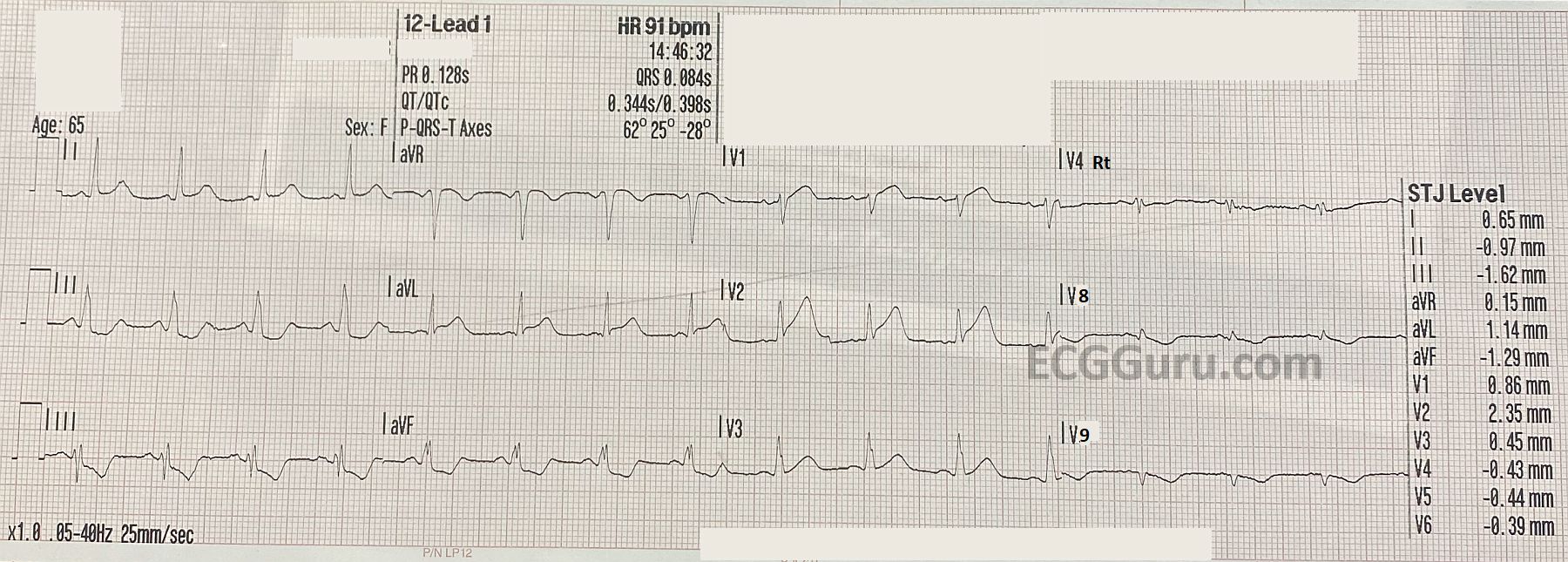
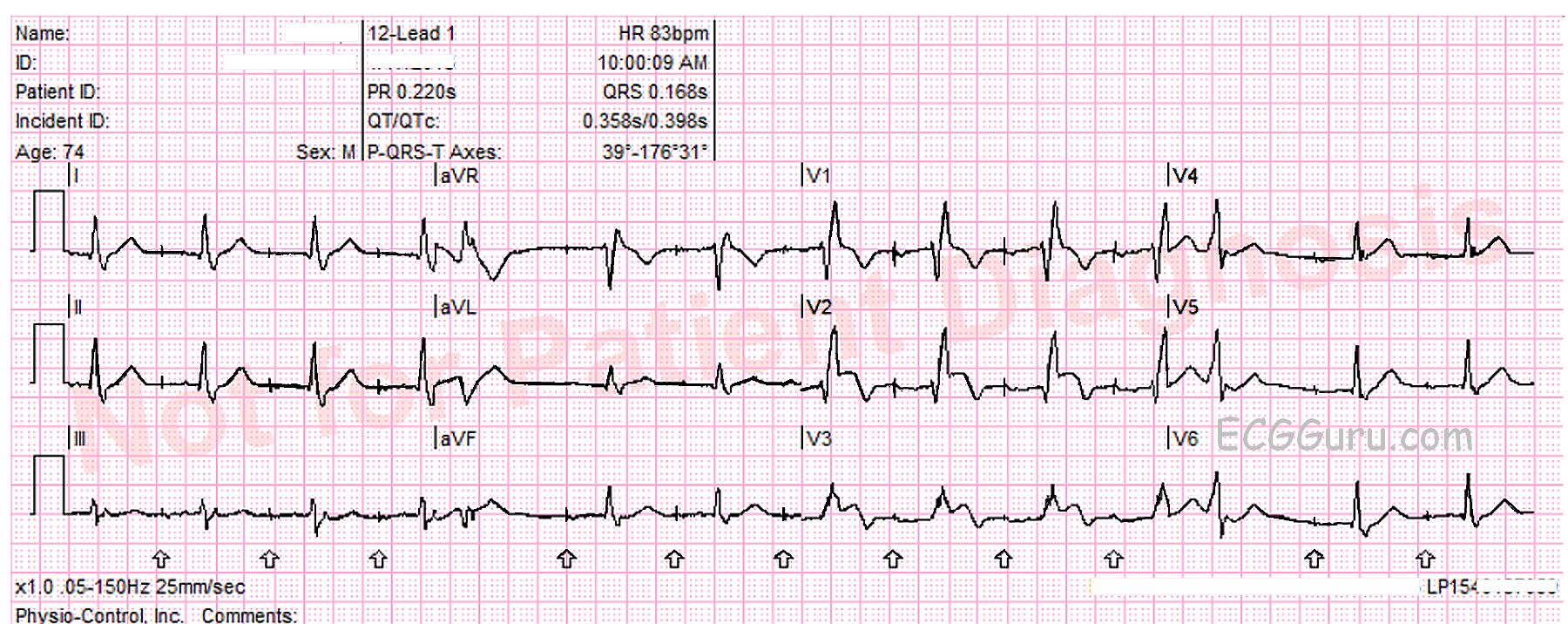
What does the ECG show? The ECG shows an atrial paced rhythm, with two premature beats, beats number 5 and 12. These are probably PVCs. The patient has a functioning AV conduction system, so the paced atrial beats are conducting through the AV node and producing QRS complexes. In the interventricular conduction system, the impulse encounters right bundle branch block. This causes each QRS to have an “extra” wave attached at the end, representing slightly delayed depolarization of the right ventricle. Instead of an “rS” pattern in V1, for example, we see “rSR’ “. The slight delay causes the QRS to be widened, as we are measuring the two ventricles separately, rather than synchronously.
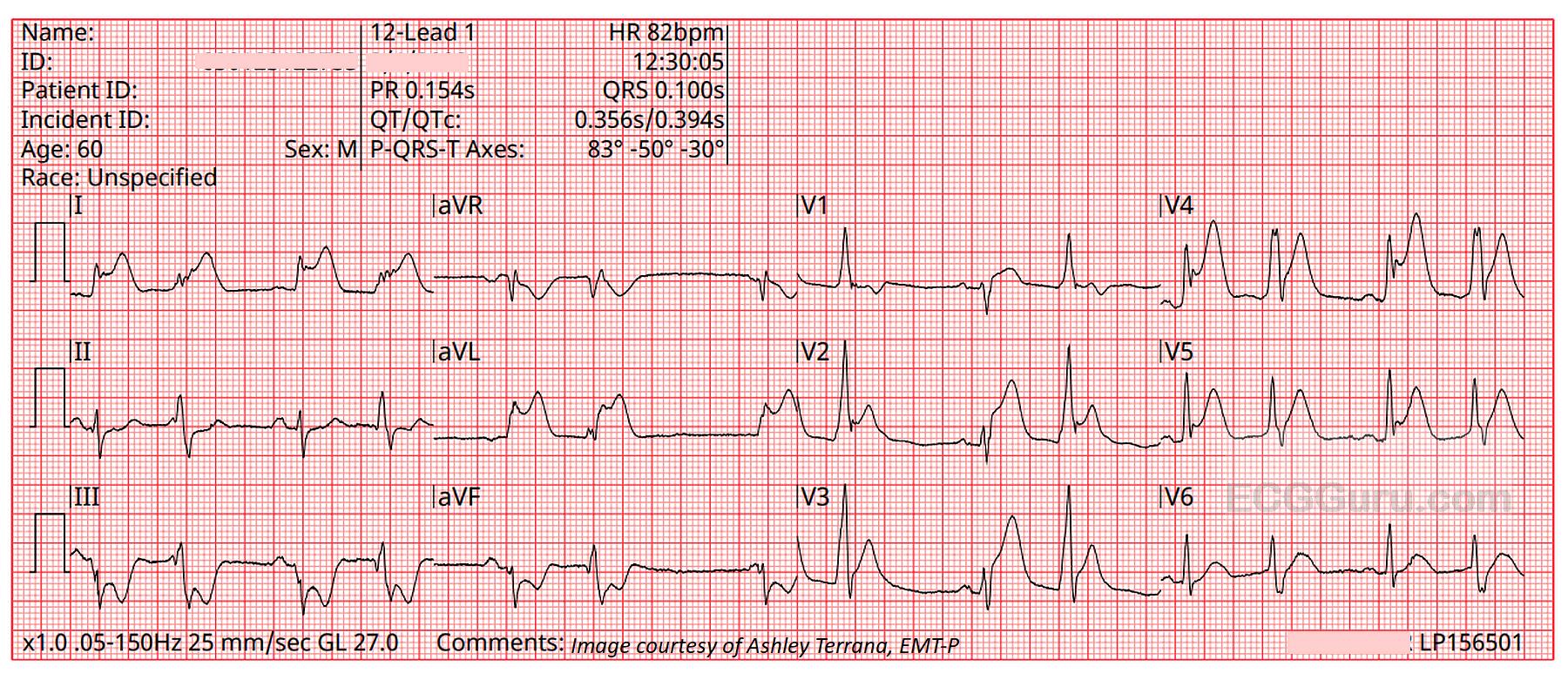
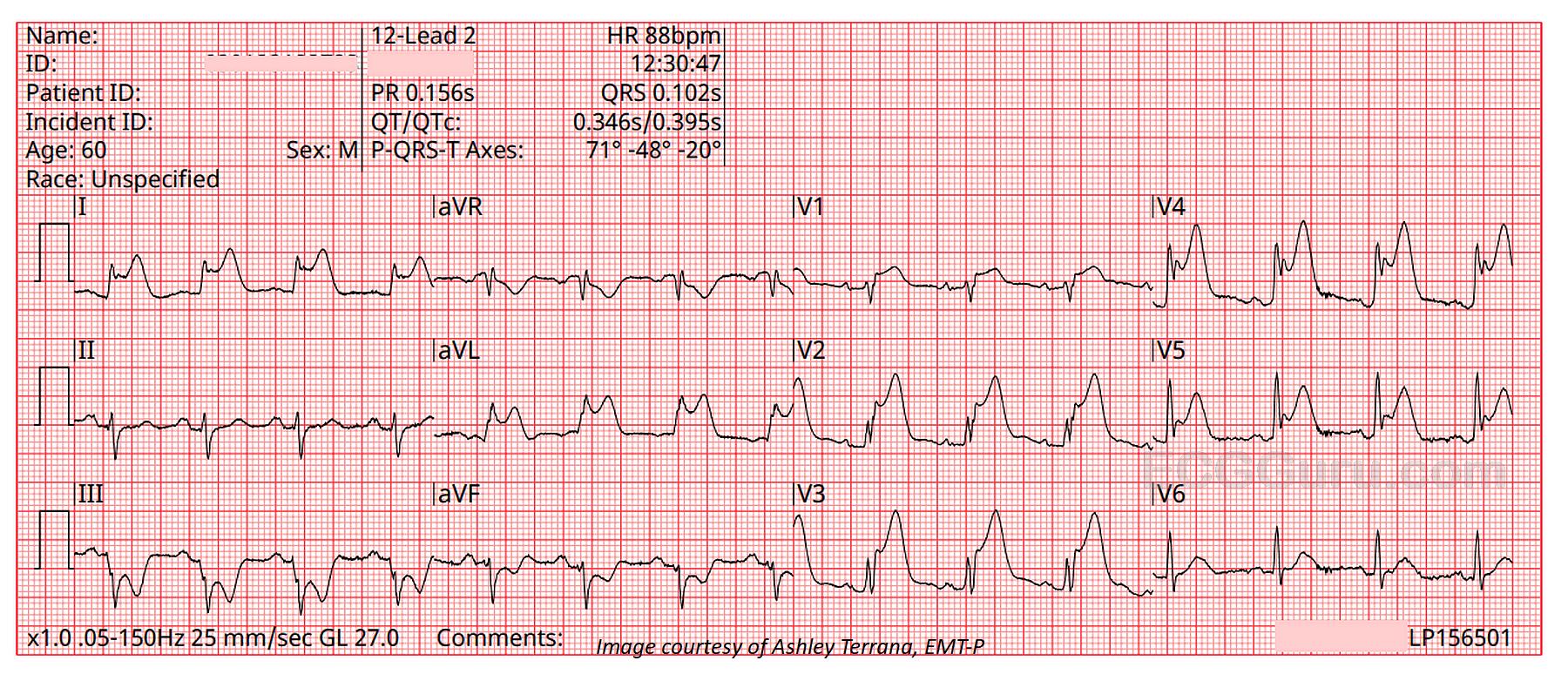
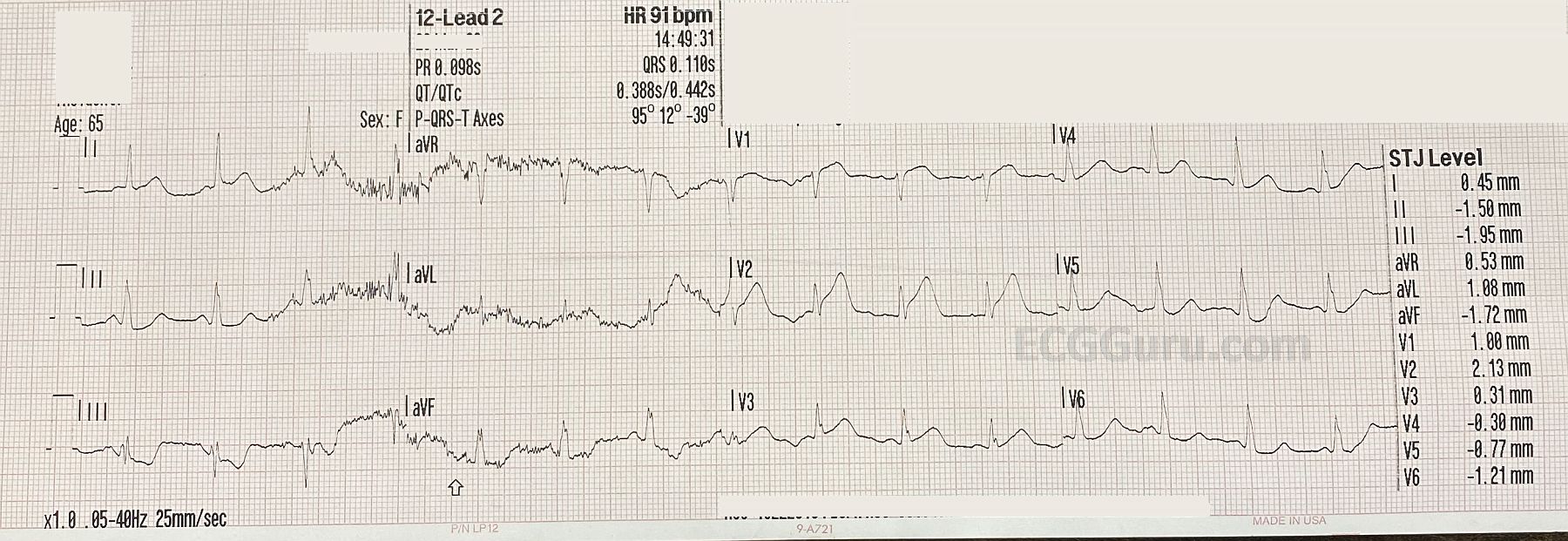
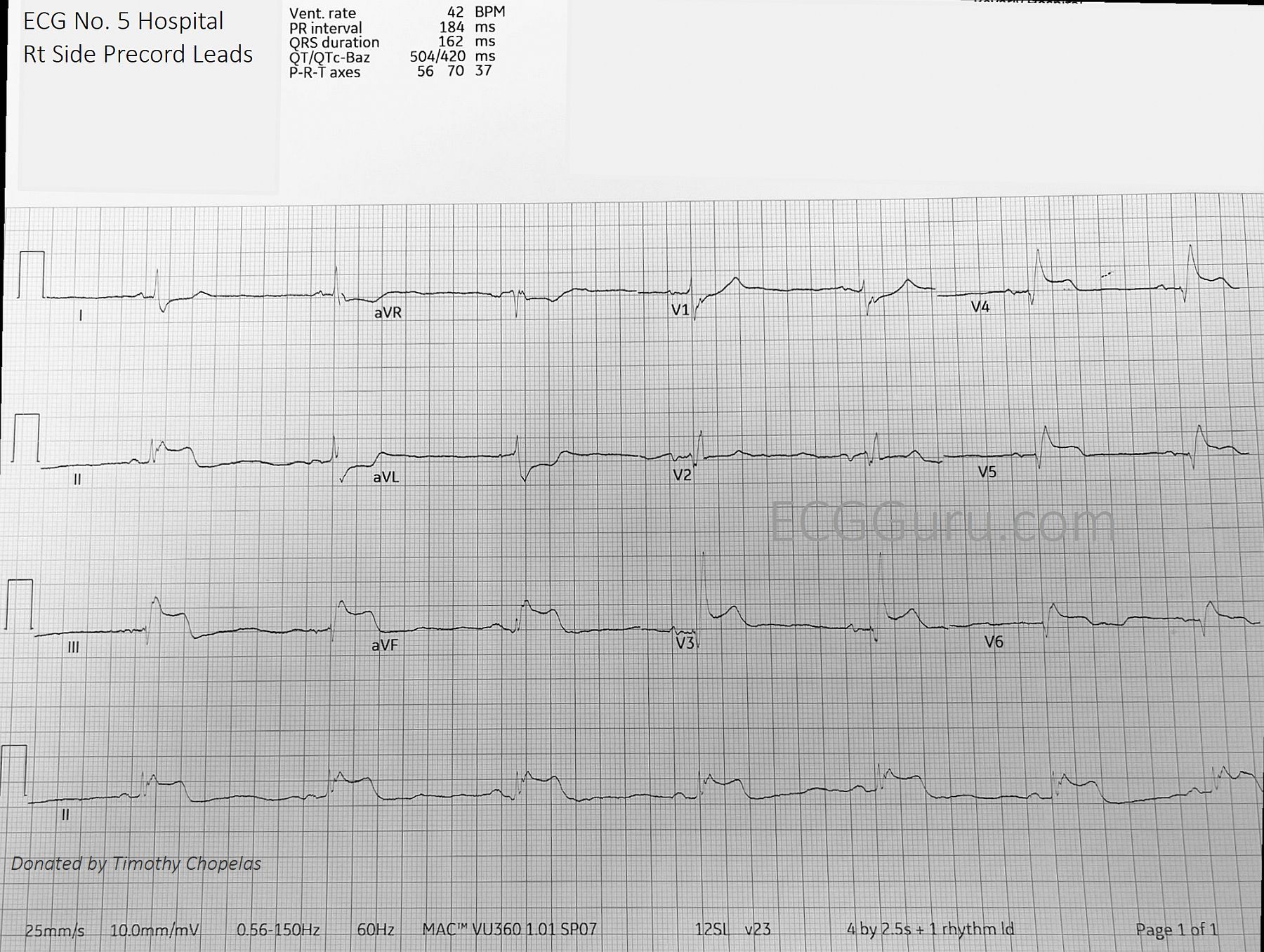
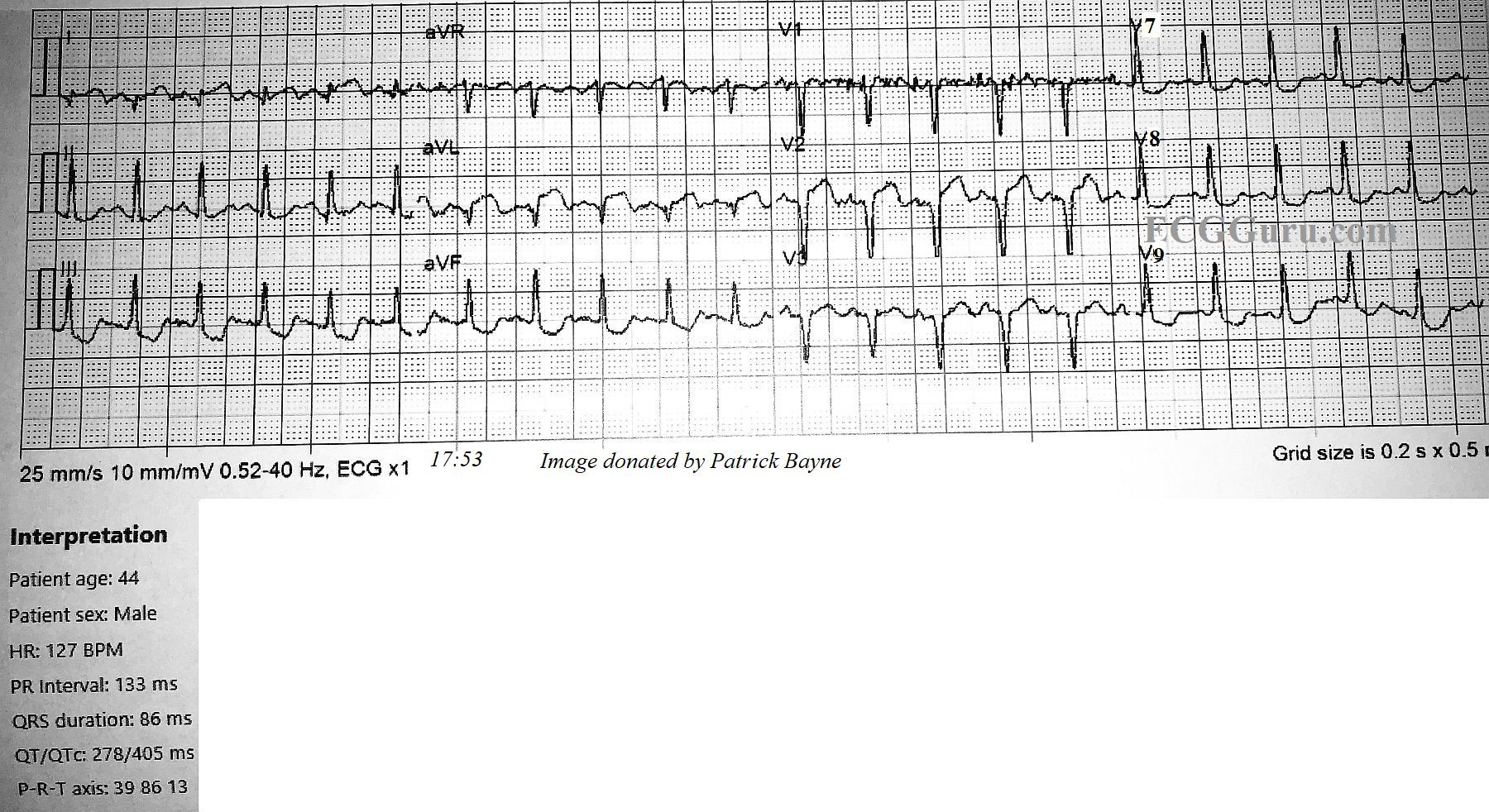
There is definite ST segment elevation in V2 and V3, and the shape of the ST segment is straight, having lost it’s normal “concave upward” appearance. In an ECG taken three minutes later, the STE extends to V4.
Do the pacemaker or the right bundle branch block prevent us from diagnosing an ST-elevation M.I.? The answer to that is a resounding “NO!” Pacemakers can sometimes make it difficult to assess ST elevation because ventricular pacing causes ST segment changes. Pacing the right ventricle causes a depolarization delay in the left ventricle as the impulse travels “cell to cell” across the LV. This means an RV-paced beat will resemble a PVC from the RV. When LV depolarization is altered, repolarization will also be altered, causing ST elevation in leads with negative QRS complexes, and ST depression is leads with upright QRSs. These are called discordant ST changes. These changes are proportionate to the height or depth of the QRS, with very minimal or no ST changes in leads with short or biphasic QRS complexes. We don’t have to worry about that in this situation – the pacemaker is not pacing the ventricles.