The patient: This ECG is from an 87-year-old man who was transported to the Emergency Department by paramedics. His chief complaint, as reported by caregivers, was lethargy, fever, and a declining mental status. He appeared tired and slightly confused, and was normotensive.
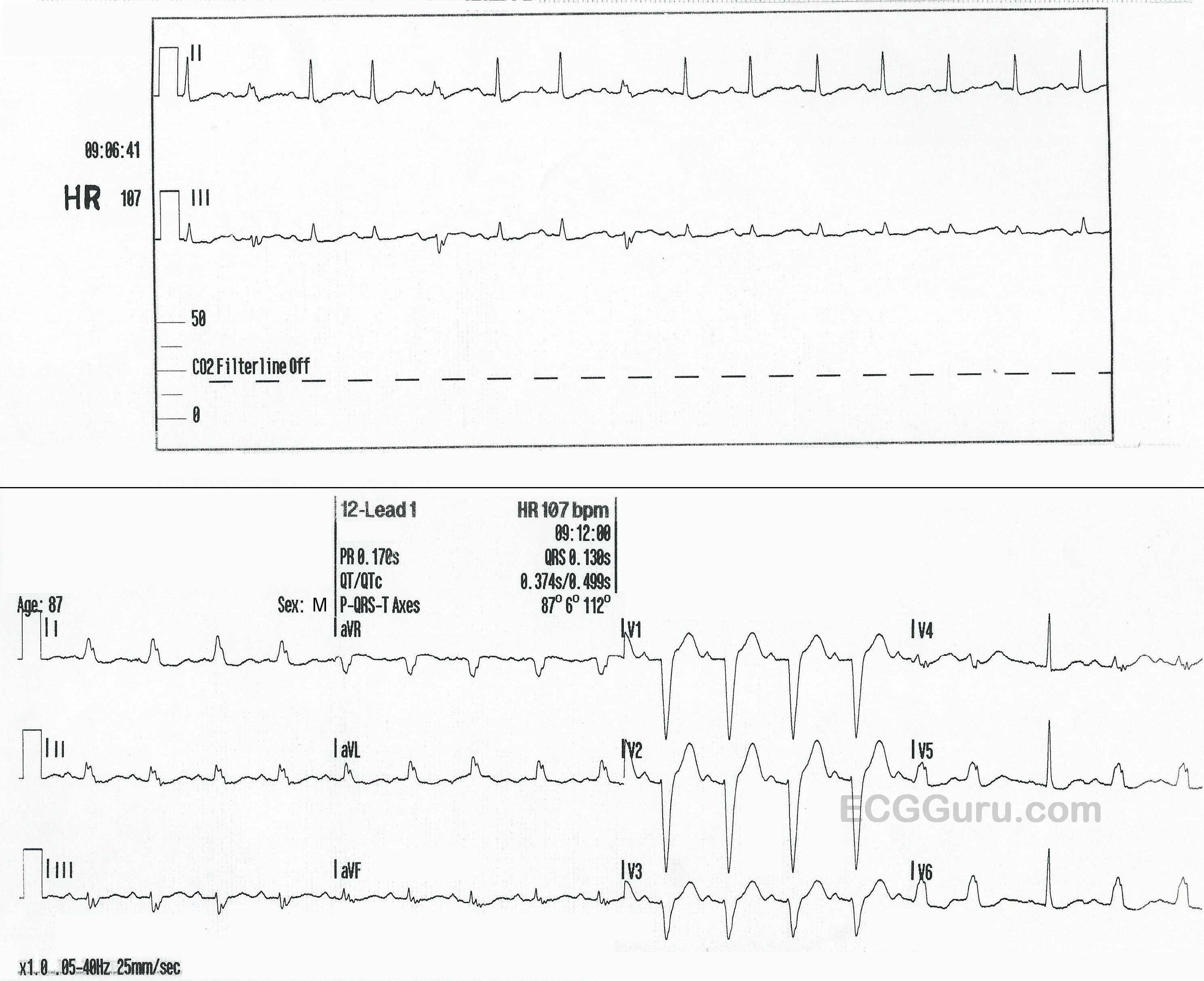
The ECG: There are a rhythm strip with two leads, II and III, and also a standard 12-lead ECG. The RHYTHM STRIP shows a tachycardiac rhythm that slows very slightly toward the end. The rate is around 107 bpm, with an R to R interval of approximately 543 ms in the earlier, regular portion. There are regular P waves present, all followed by QRS complexes. Most of the QRS complexes are normal width, but the 2nd, 5th, and 8th are slightly wide at 130 ms, or .13 seconds.
These wider QRS complexes represent aberrant conduction with LBBB occurring intermittently. Aberrant conduction often occurs due to a faster heart rate, but the only clue here is the intermittent conduction disturbance seems to disappear when the rate slows very slightly. It is hard to determine mechanism of aberrant conduction when we have only a ten-second rhythm strip.
The 12-LEAD ECG has essentially the same rate and rhythm, except all the beats in the first ¾ of the ECG are conducted aberrantly, in a LEFT BUNDLE BRANCH BLOCK pattern. This indicates that the LBB is refractory at this time. Beat No. 15 is premature (PAC). The pause after the PAC allows the left bundle branch to repolarize, conducting one single beat normally.