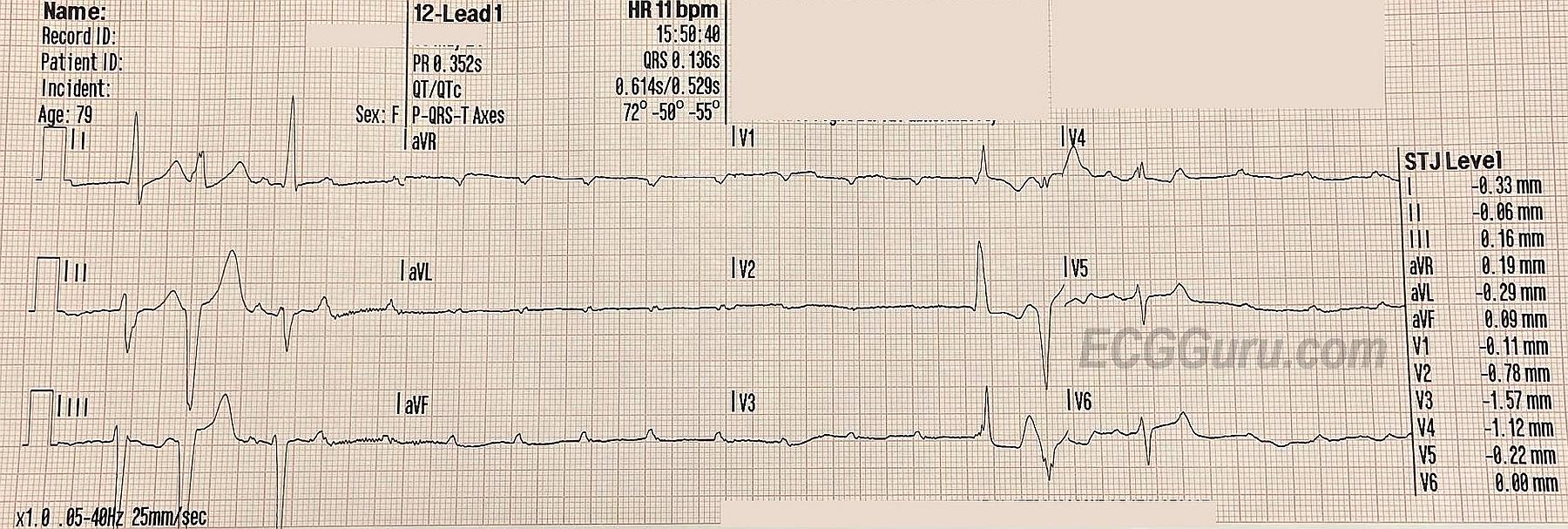
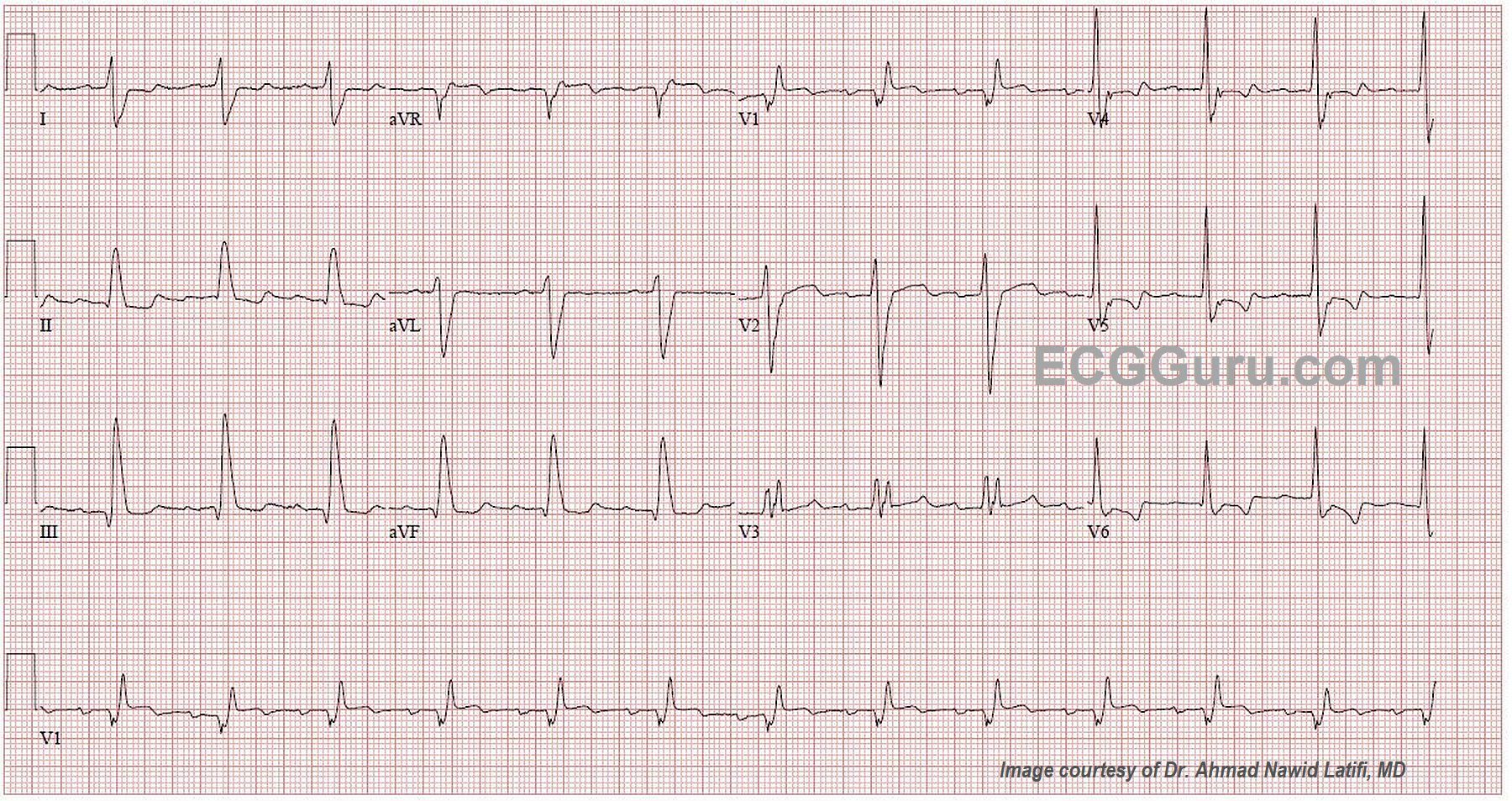
This ECG was obtained from an 84-year-old woman who was scheduled for surgery. When the anesthesiologist did this ECG, the surgery was cancelled. It is a very good example of fascicular-level blocks.
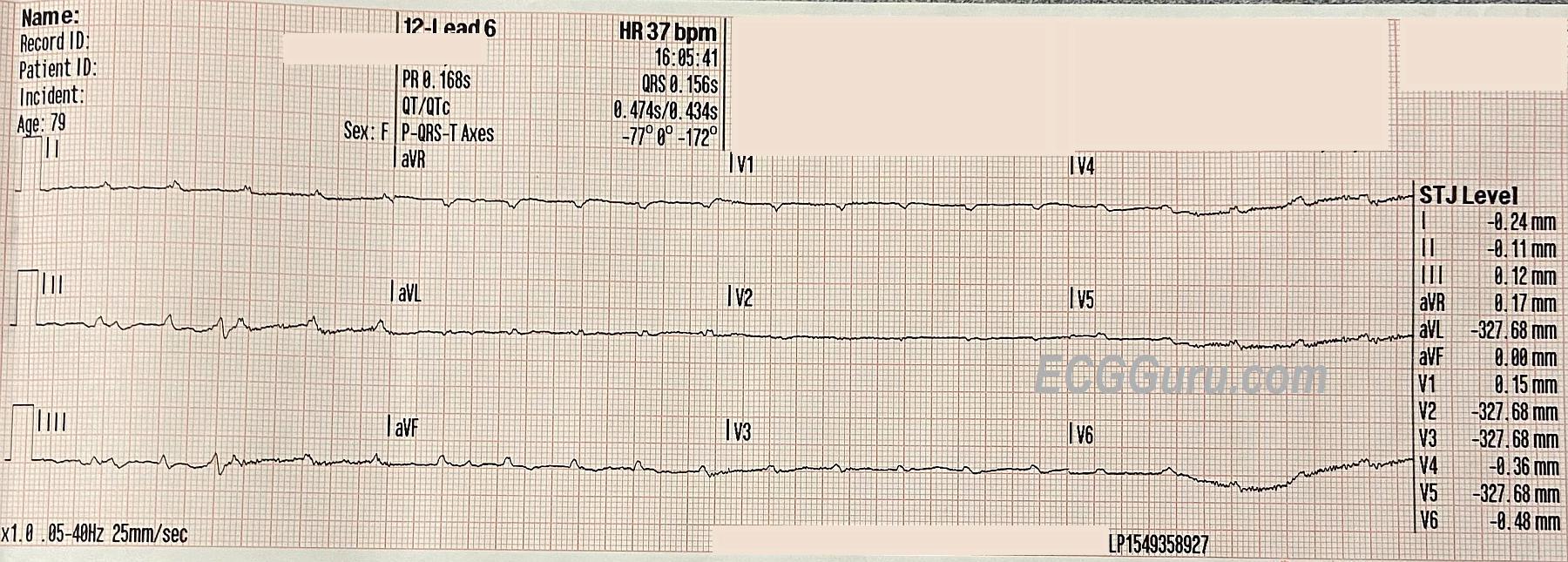
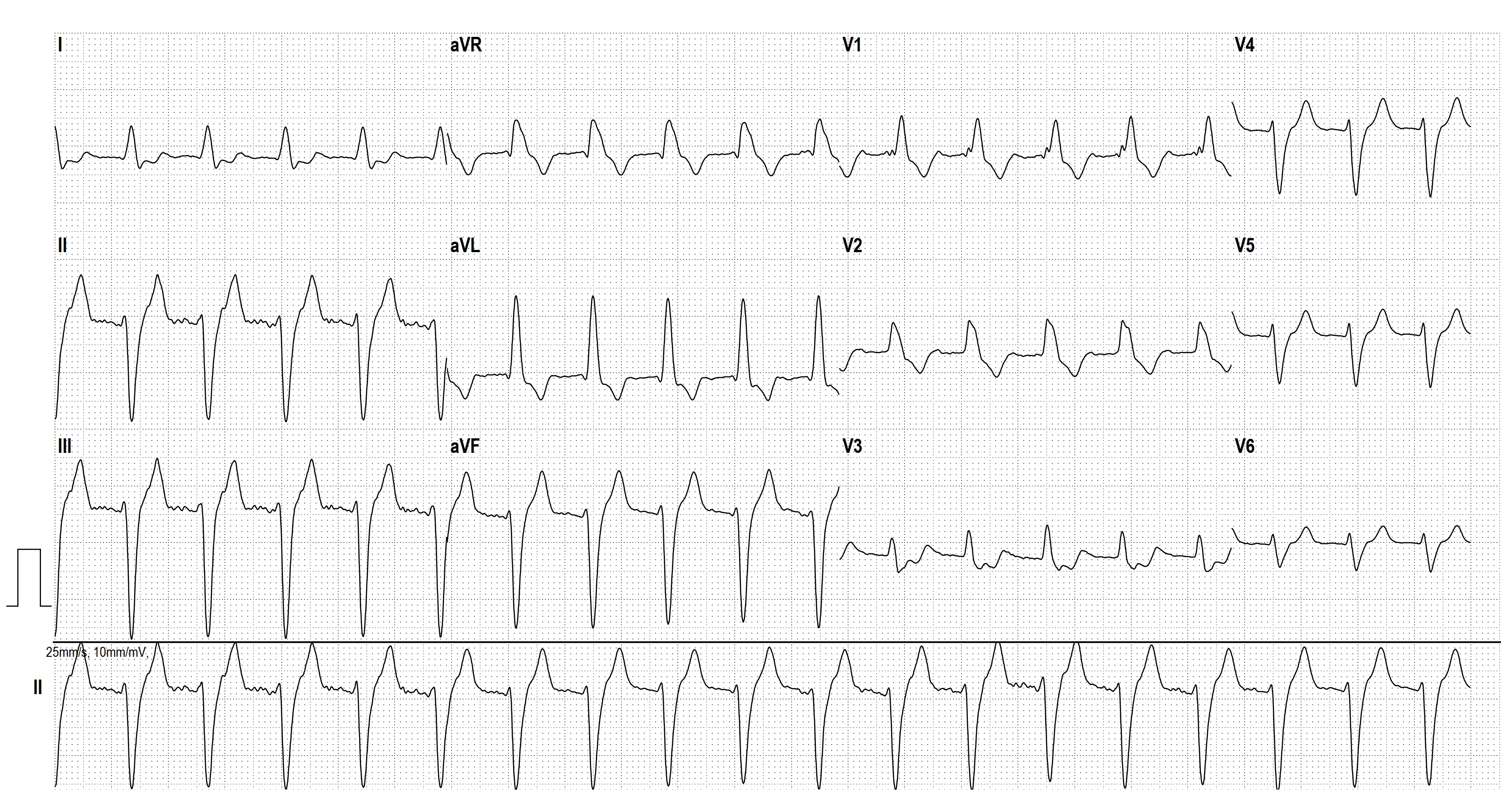
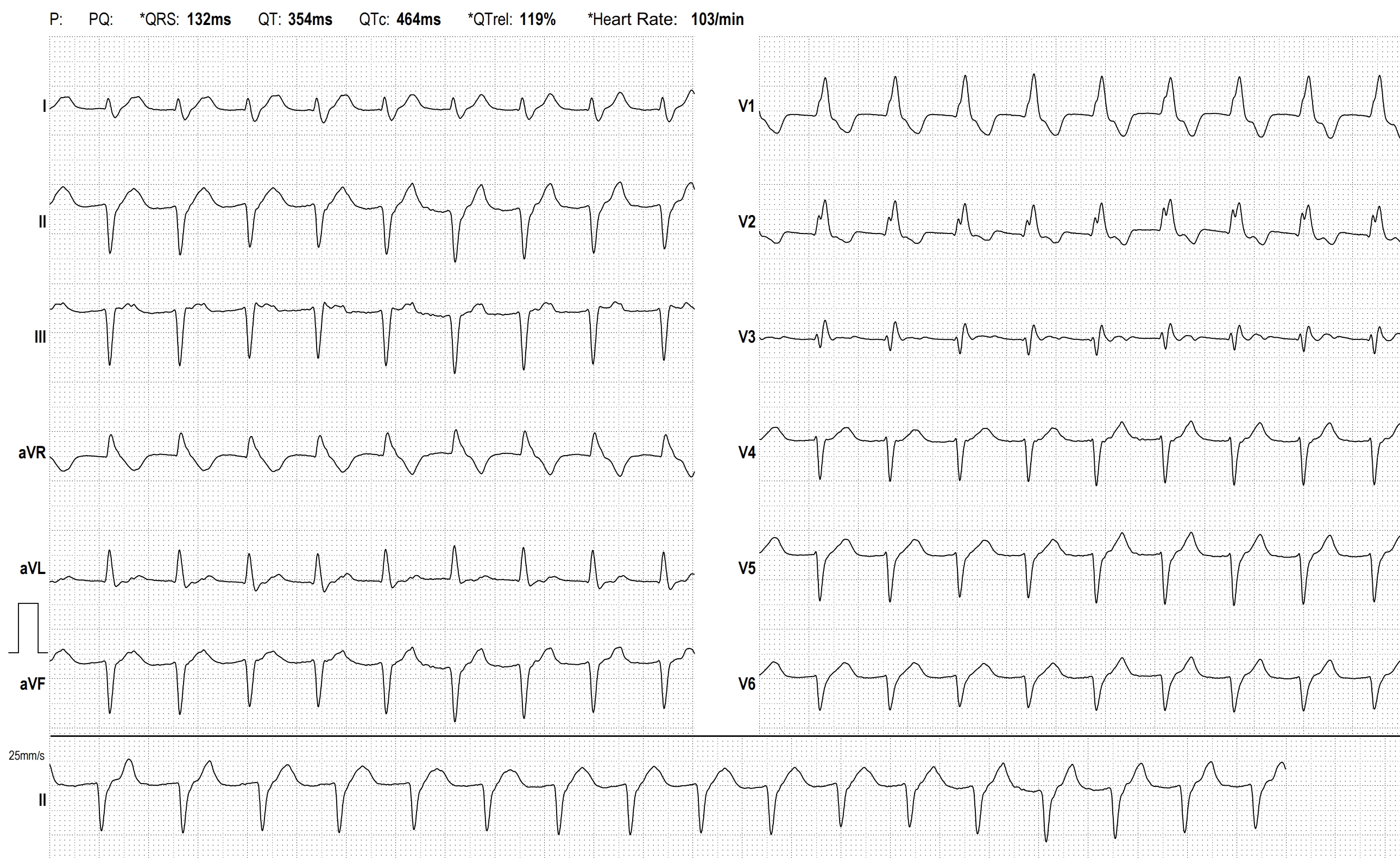
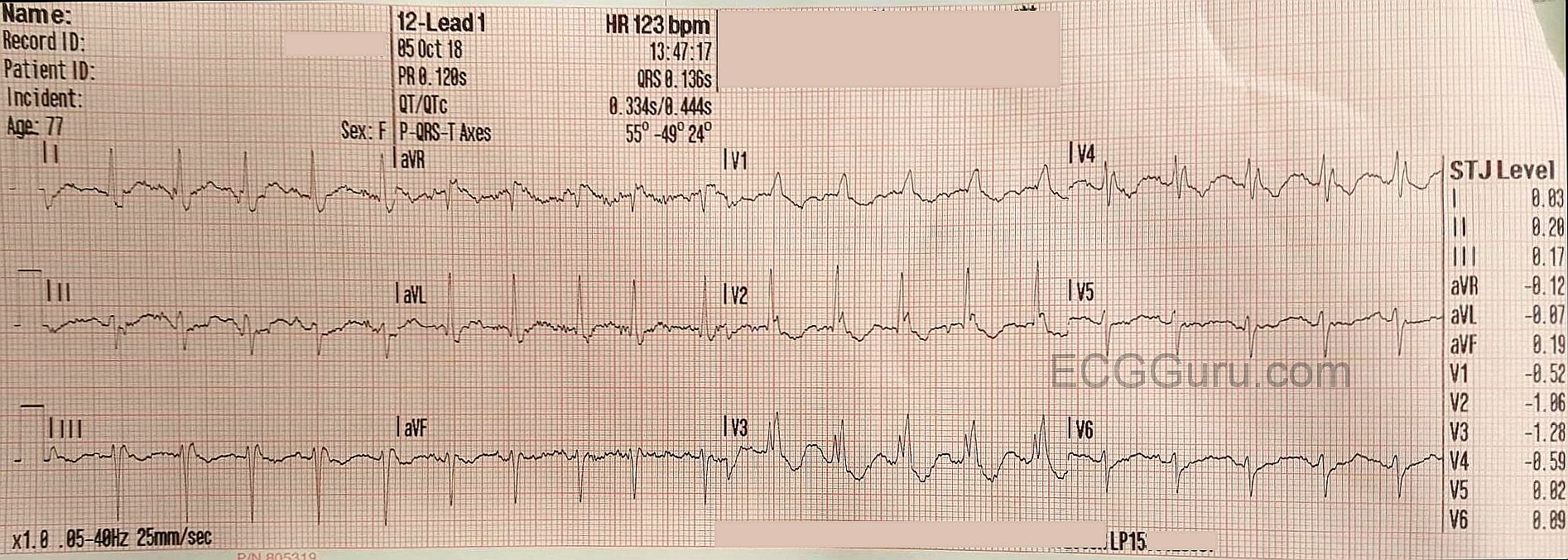
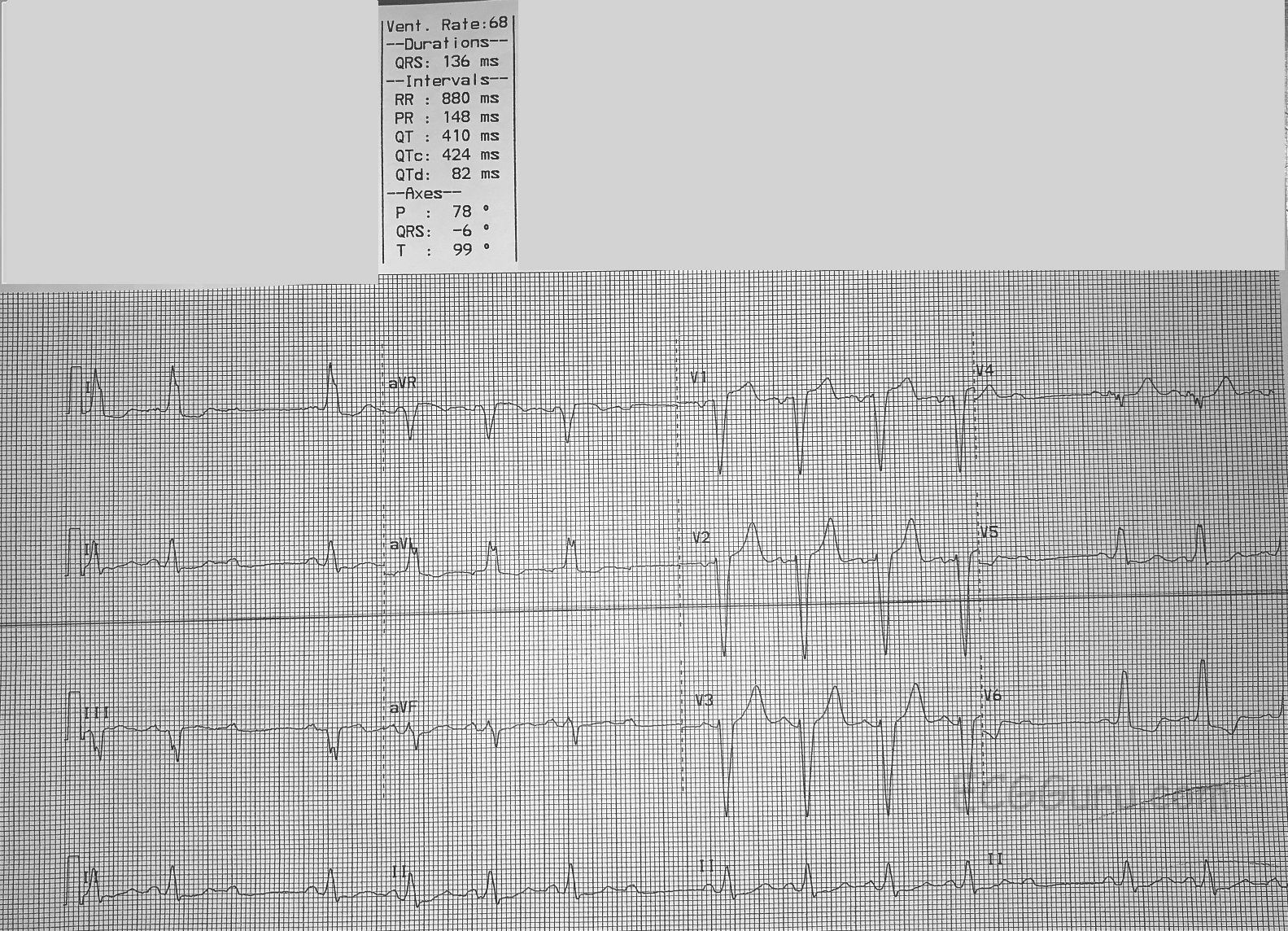
The underlying rhythm is a regular sinus rhythm at about 95 bpm. There are some non-conducted P waves which are part of the sinus rhythm (not premature beats). When the P waves DO conduct, the PR interval is steady at about .15 seconds (148 ms).
In addition, there is a LEFT BUNDLE BRANCH BLOCK. The ECG criteria for LBBB are: 1) A supraventricular rhythm, 2) A wide QRS, and 3) A negative QRS in Lead V1 and a positive QRS in Leads I and V6. The QRS duration in this ECG is 136 ms.
There are generally two fascicles (branches) in the left bundle branch, and one main fascicle in the right bundle branch. So, a LBBB represents a “bi-fascicular block”. That means that A-V conduction is proceeding down only one fascicle (the right bundle branch). In that fascicle, there is an “intermittent” block. When the RBB is not blocked, we see a QRS. When it is blocked, we see none. This is then termed an “intermittent tri-fascicular block” – otherwise known as SECOND-DEGREE AV BLOCK, TYPE II. Type II blocks nearly always have a wide QRS due to the underlying bundle branch pathology. You may see RBBB, LBBB, or RBBB with left anterior fascicular block (hemiblock). Very rarely, the combination might include left posterior hemiblock. The intermittent block in the “healthiest” fascicle(s) is what makes this a second-degree block, and not a complete heart block (third-degree AVB).
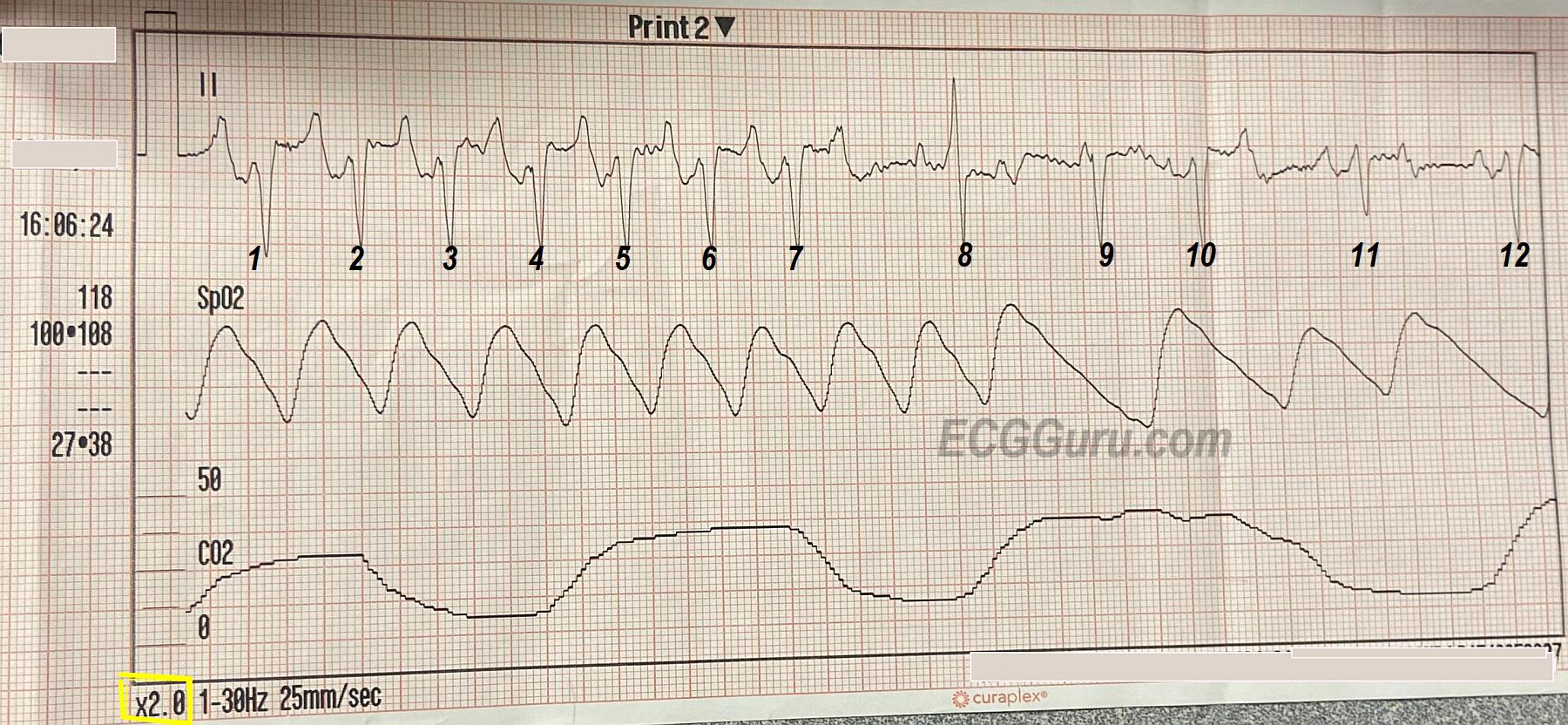
The clinical implications of this block are that the heart is operating on only one fascicle, and that fascicle is showing obvious signs of distress. A third-degree AVB could be imminent. In addition, LBBB causes a wide QRS, which decreases cardiac output. Second-degree, Type II AVBs can result in very slow rates, and sometimes cause more hemodynamic instability that some third-degree AV blocks.
This patient was scheduled for pacemaker implantation instead of the originally-scheduled surgery.