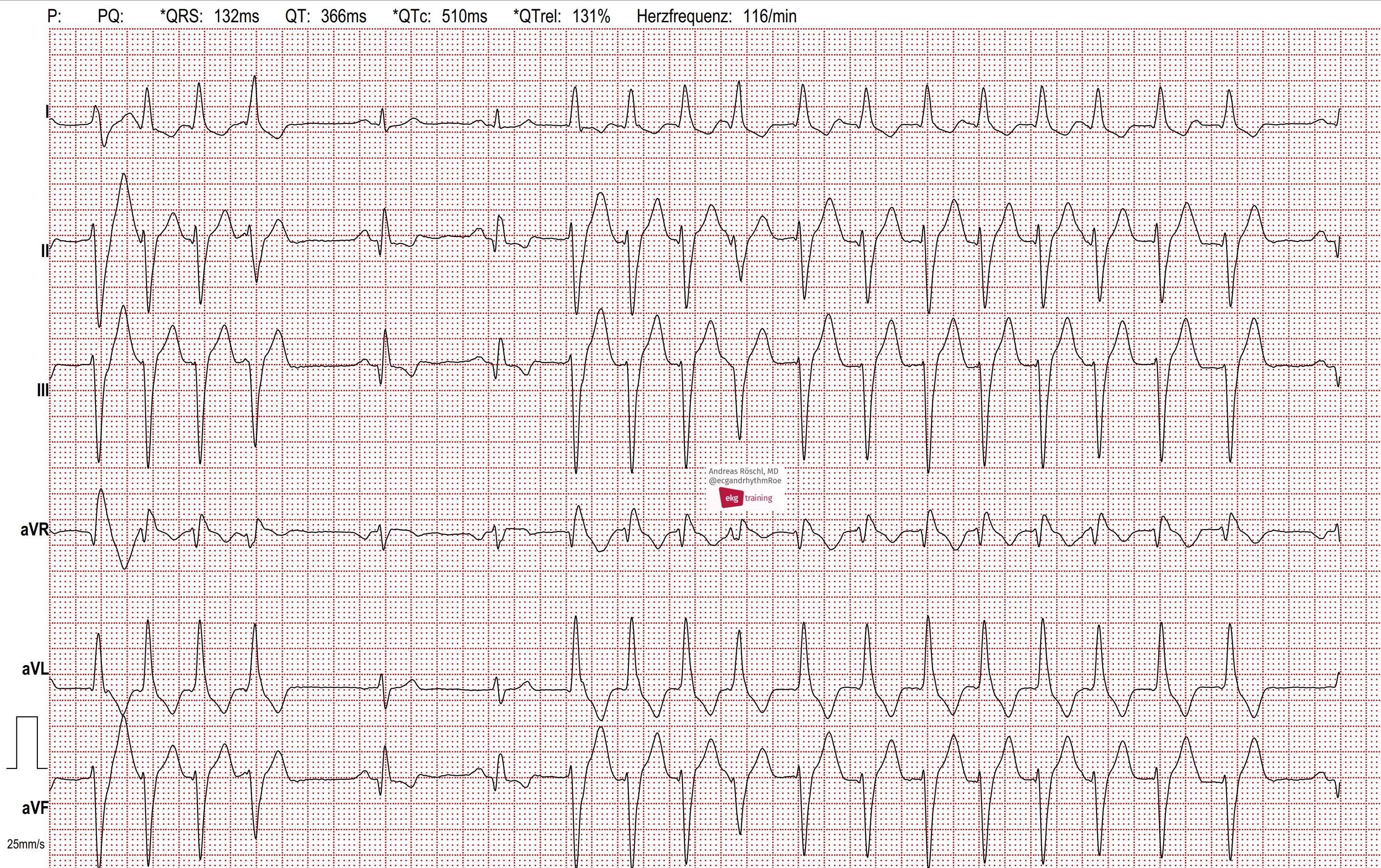
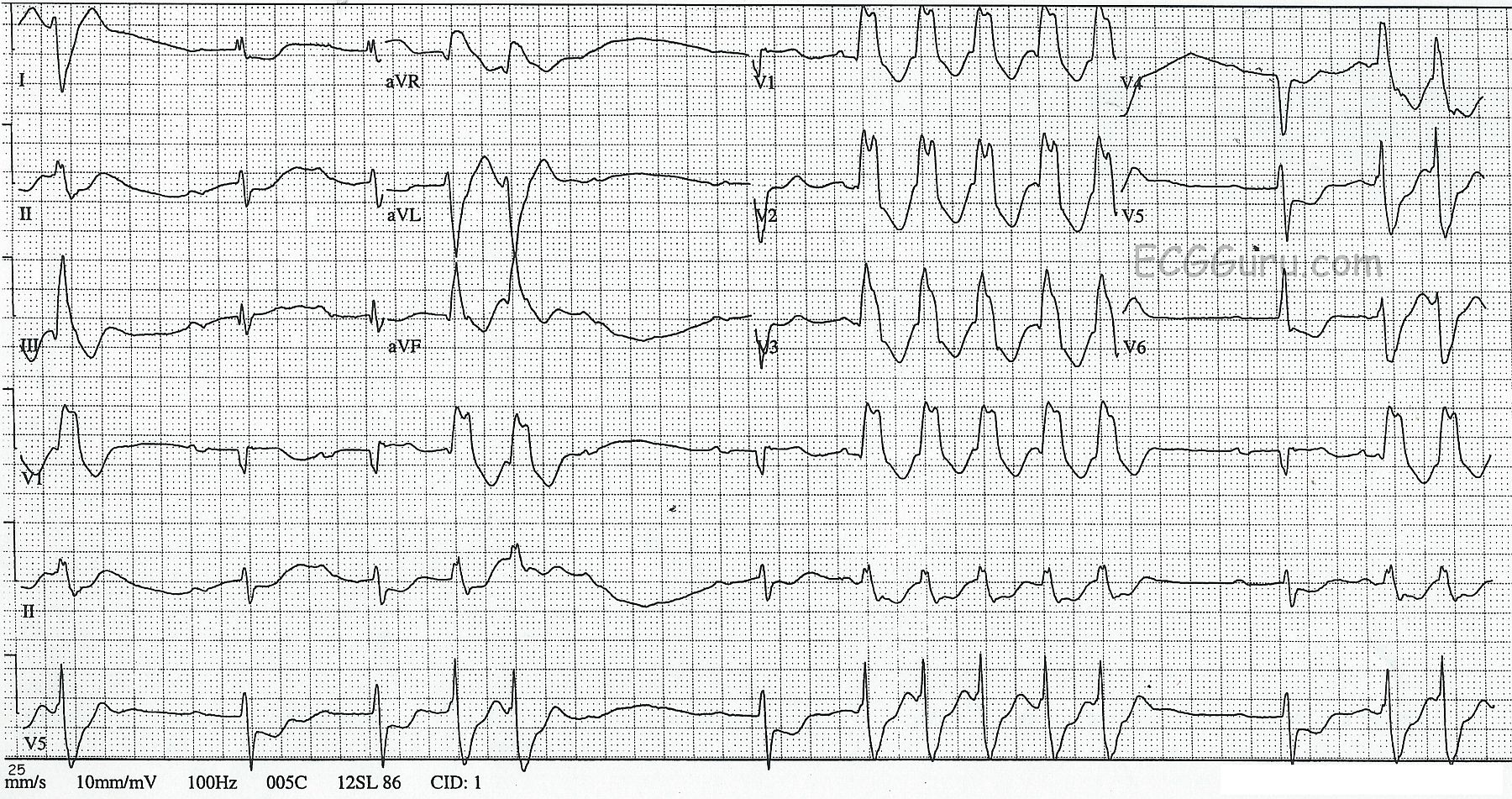
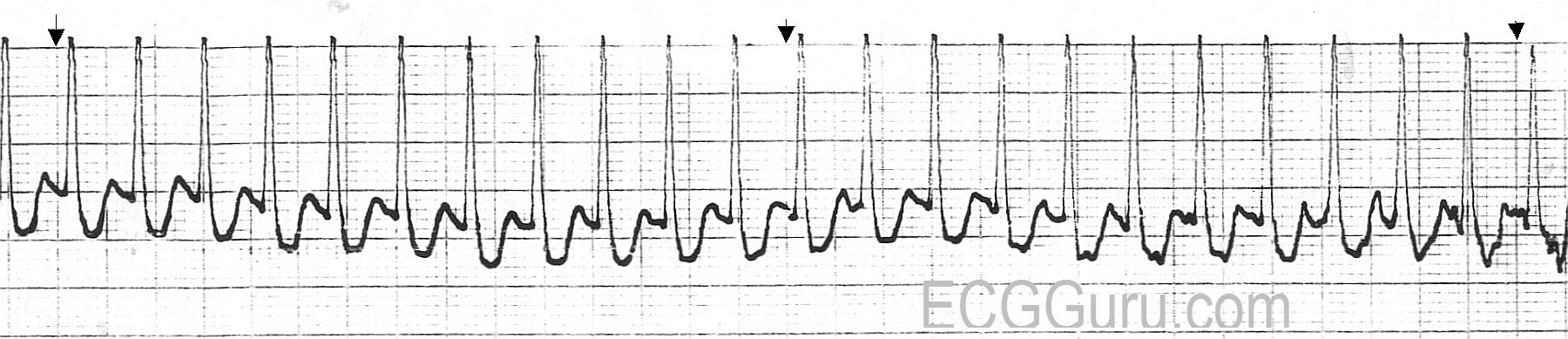
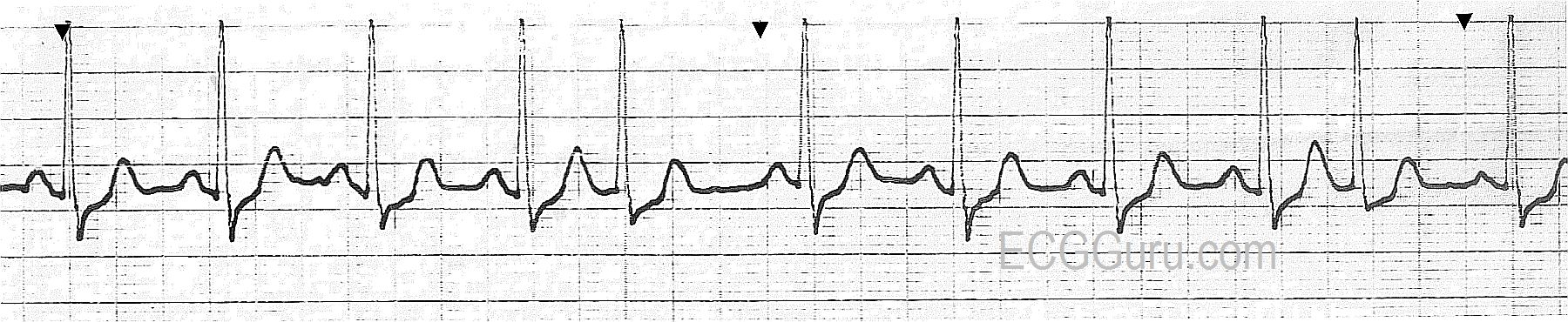
This ECG was obtained from a 45-year-old man who was experiencing palpitations and lightheadedness, which he originally attributed to anxiety. There are short, but frequent periods of ventricular tachycardia, which are self-limiting. This is called "NON-SUSTAINED VENTRICULAR TACHYCARDIA". The underlying rhythm is sinus, with a remarkably long PR interval, and at least one episode of failure of the P wave to conduct, making "second-degree AV block, Type II" a possibility. It is difficult to thoroughly evaluate the underlying rhythm because it is not seen very often in this ECG. The rate of the underlying P waves is about 67 bpm. The PR interval is .40 seconds (400 ms). The "normal" QRS complexes are slightly widened, at about .10 sec (100 ms), which is typical of Type II AVB. The ventricular QRS complexes are wide at .16 sec. (160 ms)
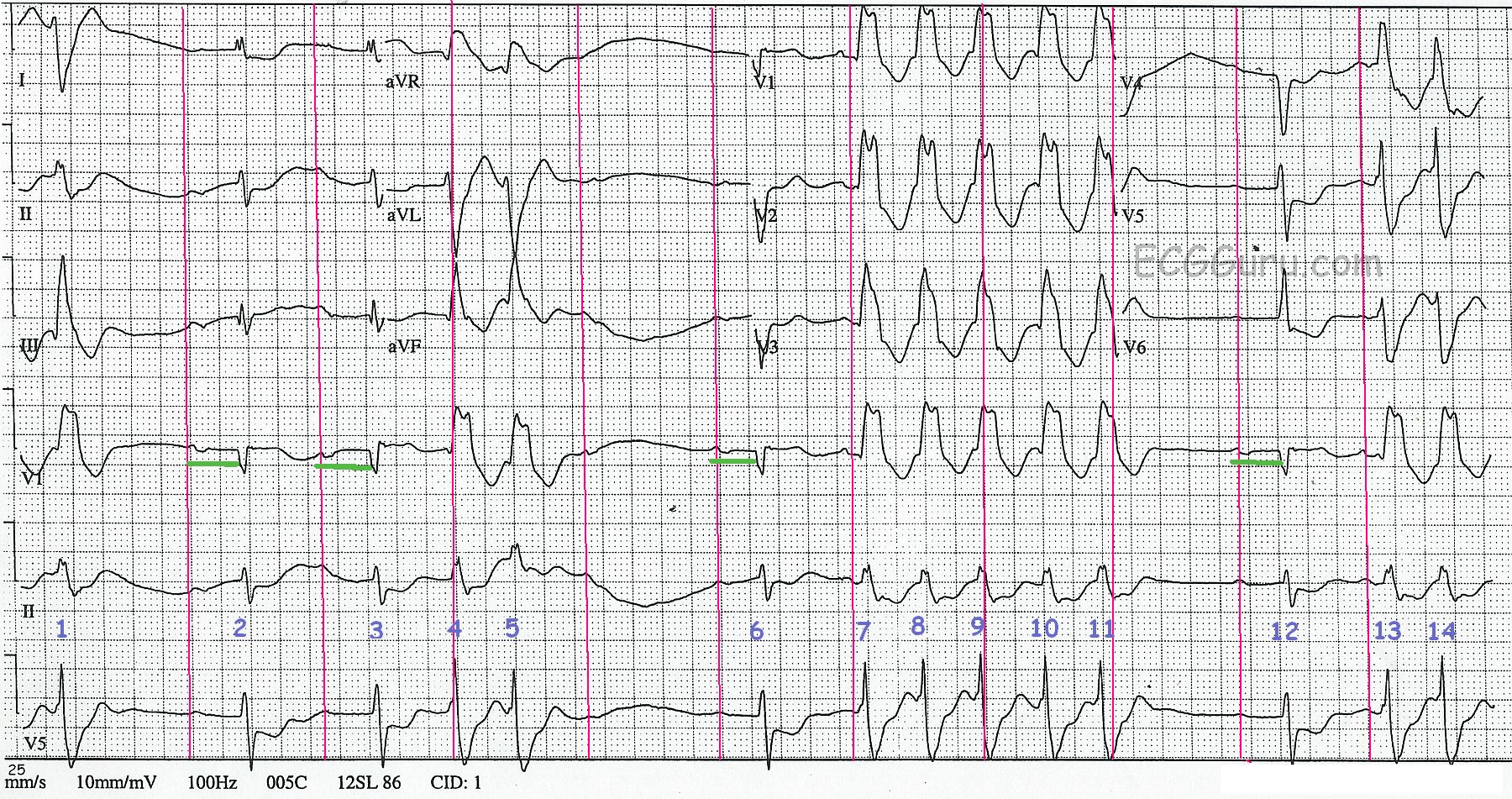
To assist you in using this tracing for teaching, we have also supplied a "marked up" version. The P waves, both visible and hidden, are marked with red lines. The PR intervals are shown in the Lead V1 rhythm strip in green. And the QRS complexes are numbered. QRS complexes numbered 2, 3, 6, and 12 are sinus. The P wave AFTER QRS #5 is non-conducted.
To review the differentiation of ventricular tachycardia from supraventricular tachycardia with aberrant conduction, go HERE.