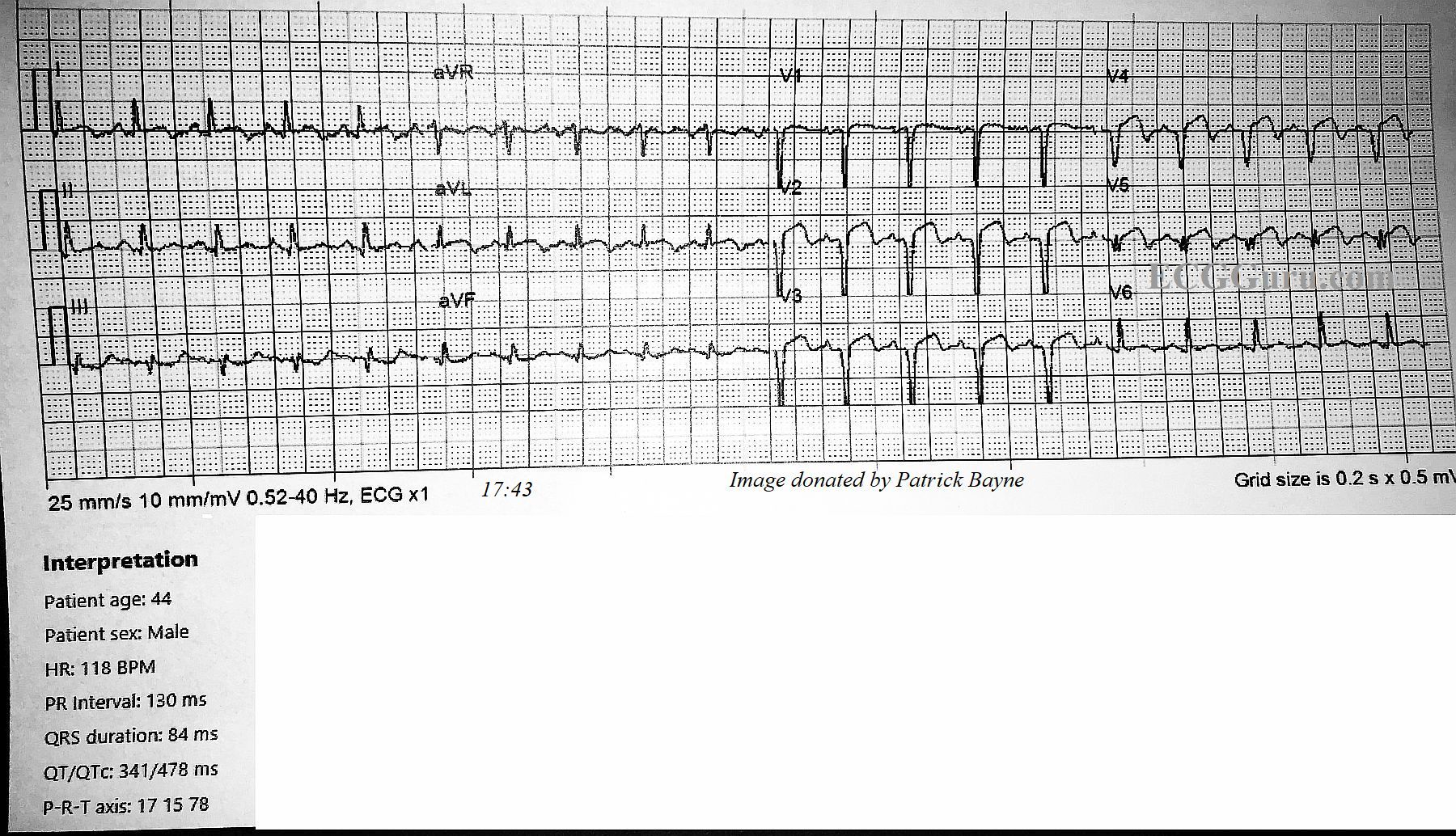
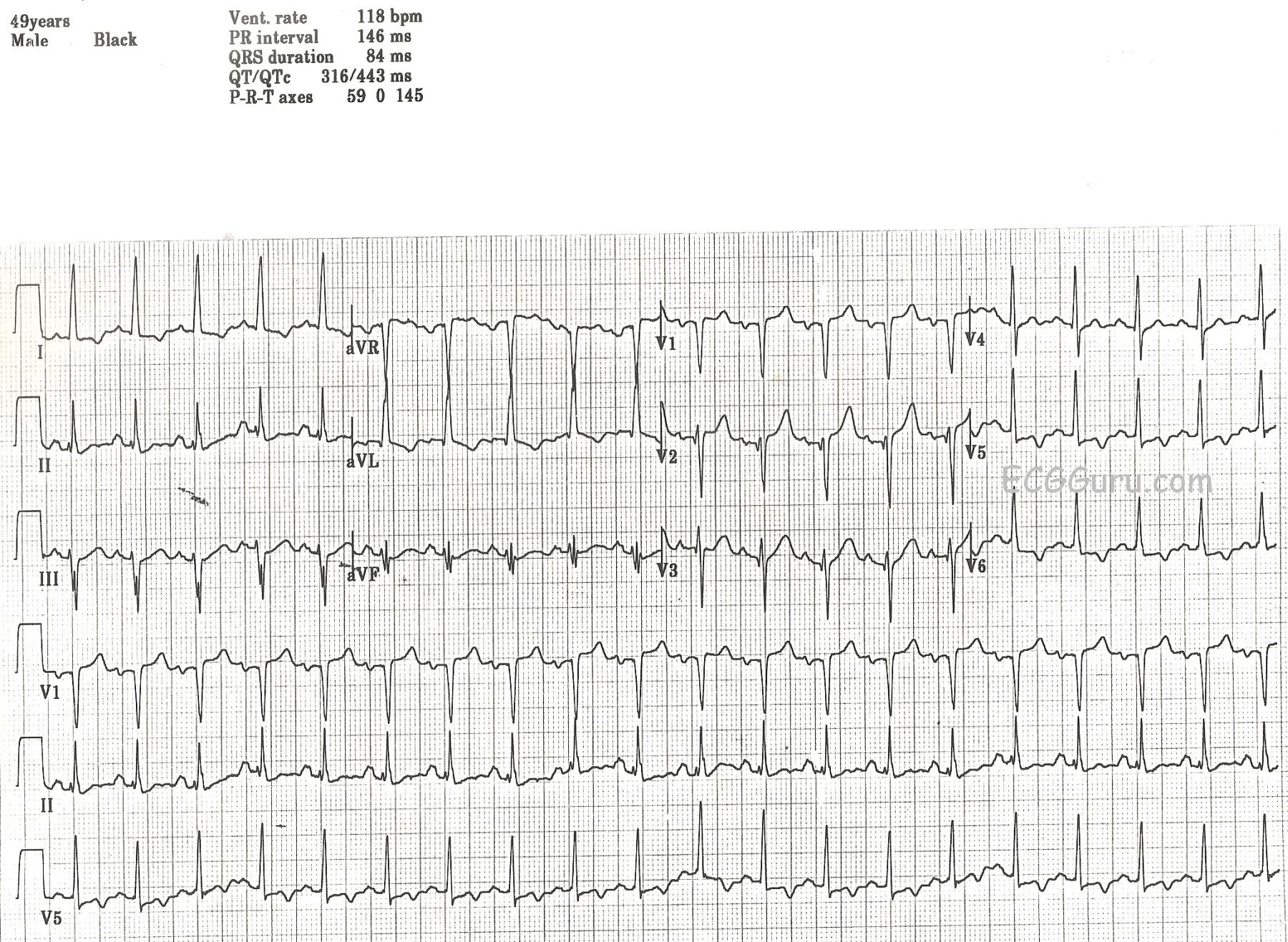
This ECG was obtained from a 49-year-old man who was a patient in an Emergency Dept. We do not know his presenting complaint, only that he had a history of insulin-dependent diabetes mellitus (IDDM). It was noted by the donor of the ECG that the patient had no chest pain, no shortness of breath, and no other cardiac symptoms. We do not know his hydration or electrolyte status. There are quite a few interesting abnormalities on this ECG, and the exact interpretation would, of course, depend upon the patient's clinical status. It would definitely help to be there!
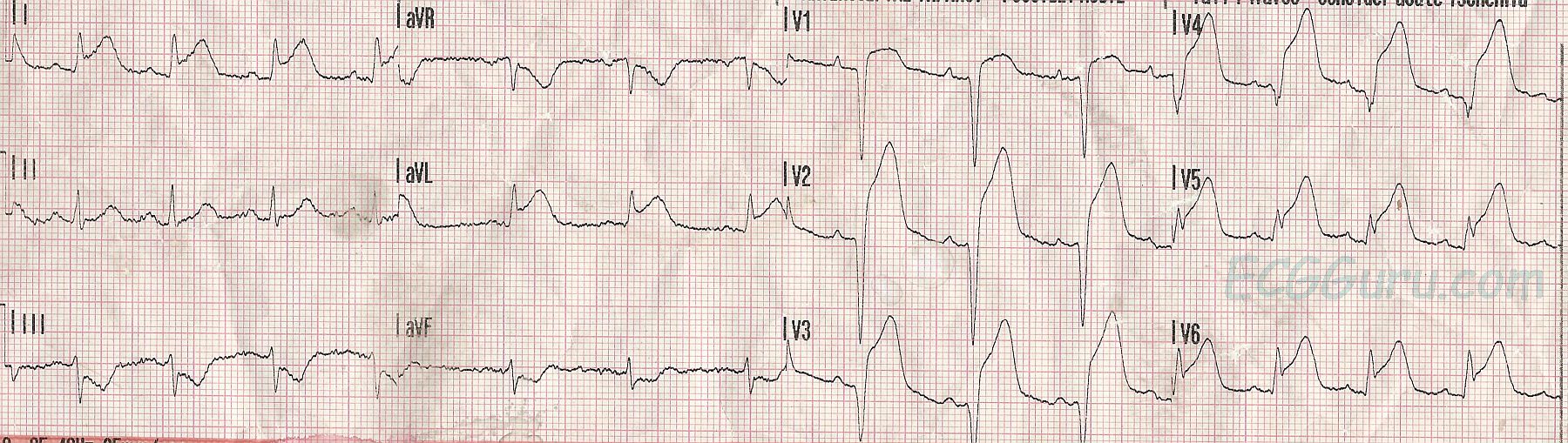
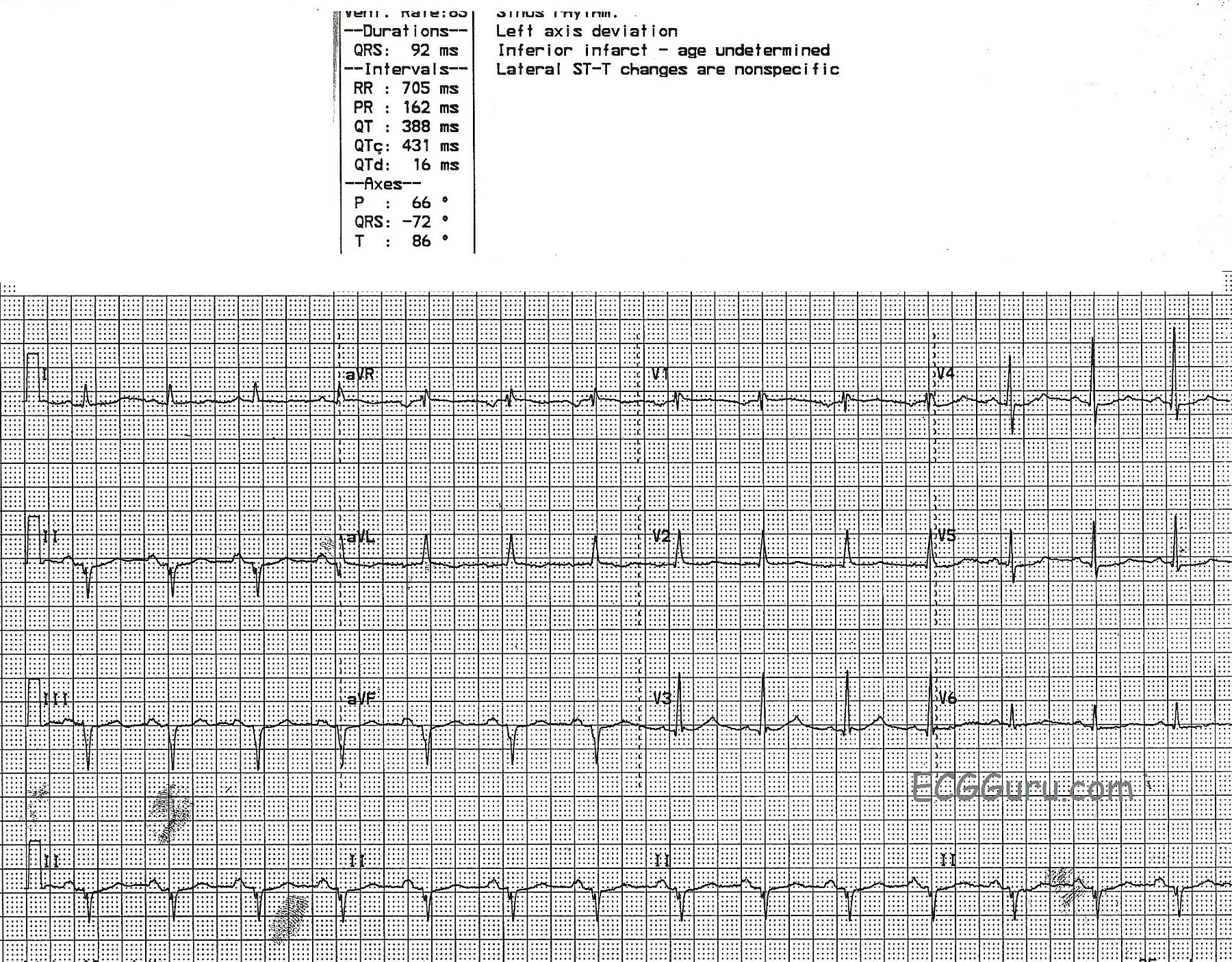
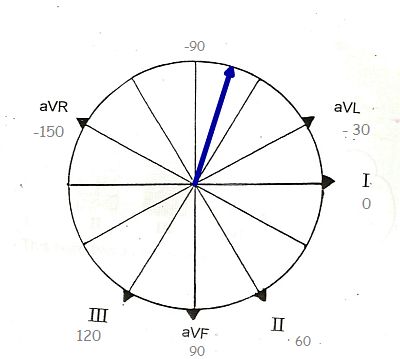
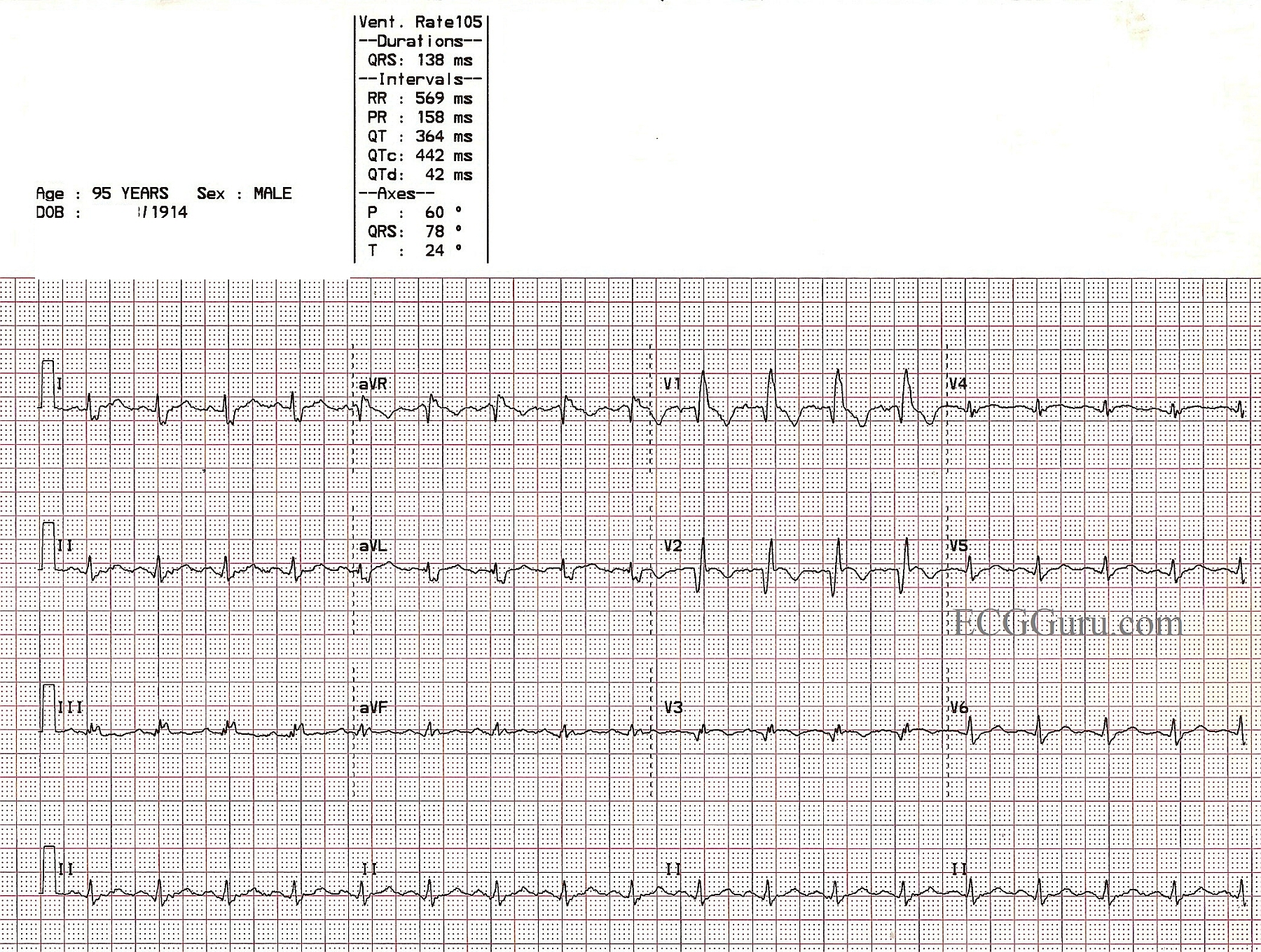
First, we note a sinus tachycardia at a rate of 118 bpm. This could be due to very many causes, including but not limited to: dehydration, pain, anxiety, high or low blood glucose, fever, or CHF. The PR and QT intervals are within normal limits. The QRS complexes are narrow. The axis is normal at 0 degrees. The QRS voltage in the lateral leads is on the high side of normal, but we do not know this patient's body type. Voltage as read by the ECG can be influenced by a thin chest (making voltage look larger) or a large chest (making voltage lower).
There are T wave abnormalities in the lateral leads: I, aVL, V5 and V6. The T waves are inverted, which can have many meanings. However, when inverted T waves are in the lateral leads, as opposed to the inferior or right chest leads, it is often a sign of ischemia. The flat, horizontal ST segments can also signify coronary artery disease (CAD). This patient denied cardiac symptoms, but his age and history of IDDM make it probably that CAD is a factor. The leads with T wave inversion also have a small amount of ST segment depression. The right precordial leads, V1 and V2, have a small amount of ST elevation, This possibly represents a reciprocal change to the ST depression in V5 and V6.
Because we are not at the bedside of this patient, there are many details we do not know. But these inverted T waves could be ischemic T waves, and this requires that the patient be further evaluated.
As always, we welcome comments, as this ECG probably has more to say!
REFERENCES: Dr. Ken Grauer, Life In The Fast Lane, World Journal of Cardiology