Submitted by Dr A Röschl on Sat, 05/27/2023 - 01:46
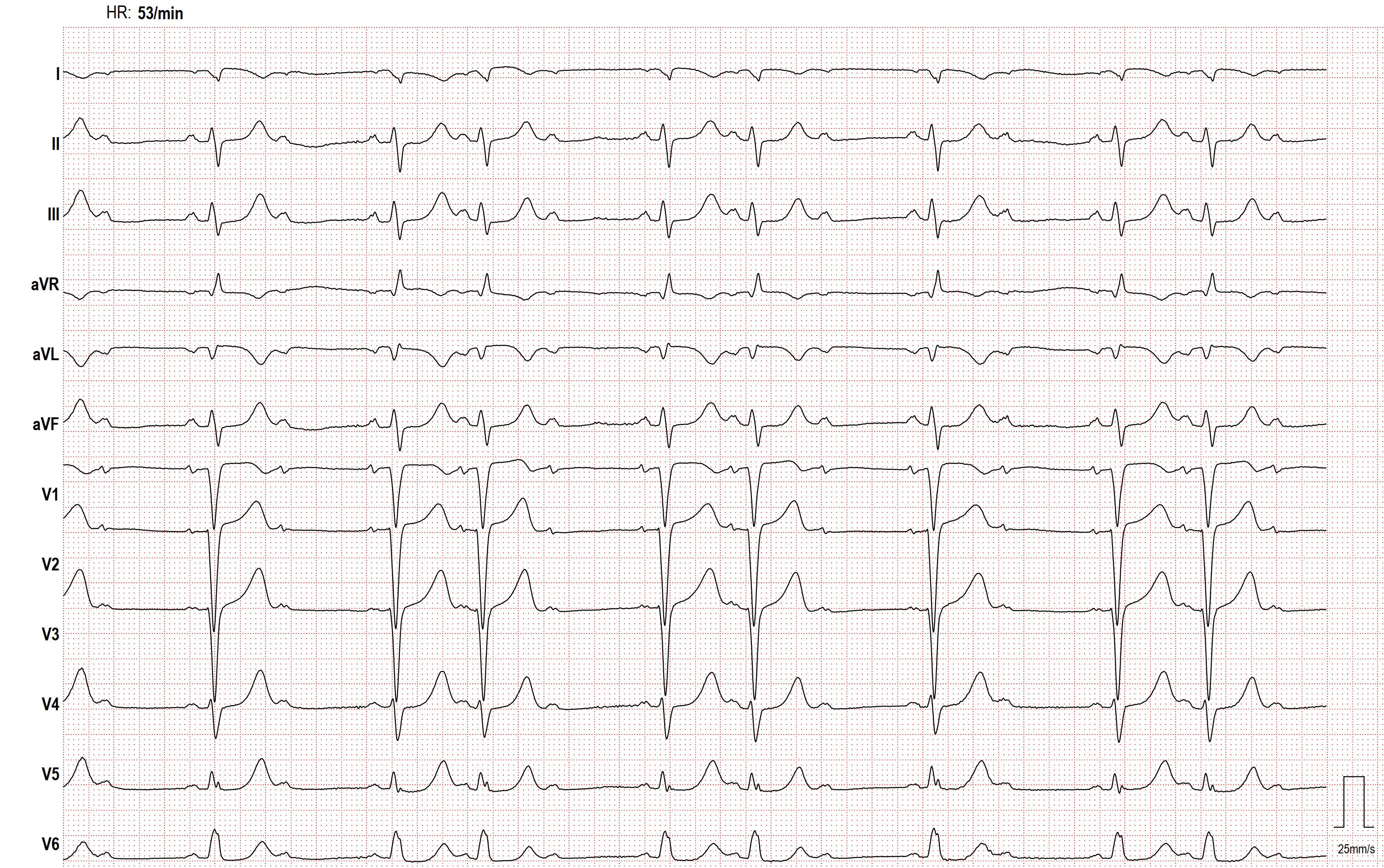
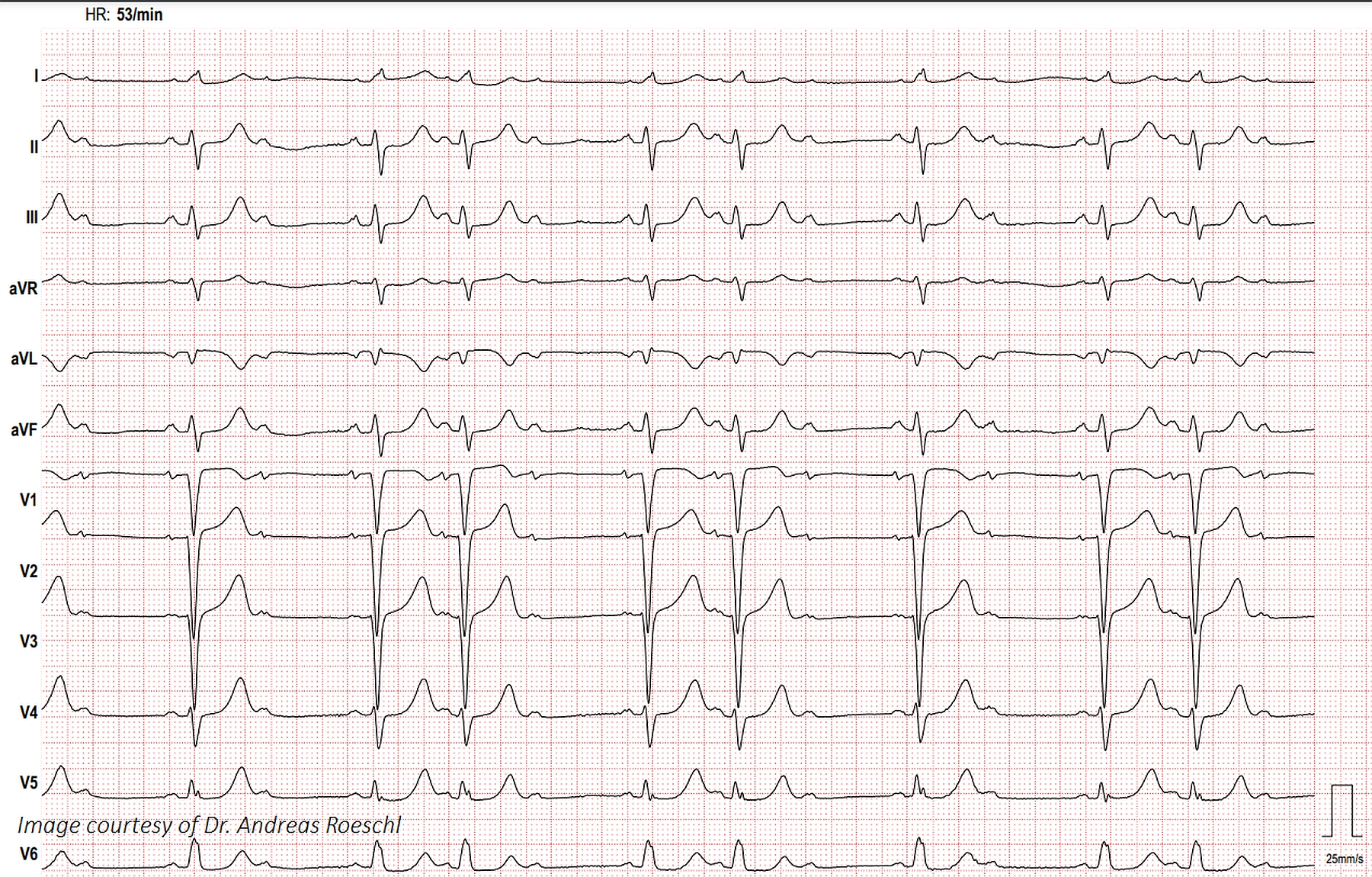
This ECG shows second-degree AV block, Mobitz Type II and an interventricular conduction delay, probably left bundle branch block. The QRS width is about 130 ms, or .13 seconds.
Dr. Jerry W. Jones, MD, FACEP, FAAEM has graciously shared with us his four-part article on the topic of “Delays & Blocks Involving the Bundle Branches”.
Dr. Jones is a talented instructor who makes difficult topics easy.Please feel free to post your comments and questions for Dr. Jones and our other ECG Gurus.
Click THIS LINK for a downloadable pdf of Part 1: Non-Specific Intraventricular Conduction Delays.
Click THIS LINK for a downloadable pdf of Part 2: Left Bundle Branch Block.
Click THIS LINK for a downloadable pdf of Part 3: Right Bundle Branch Block.
Click THIS LINK for a downloadable pdf of Part 4: The Fascicles of the Left Bundle Branch
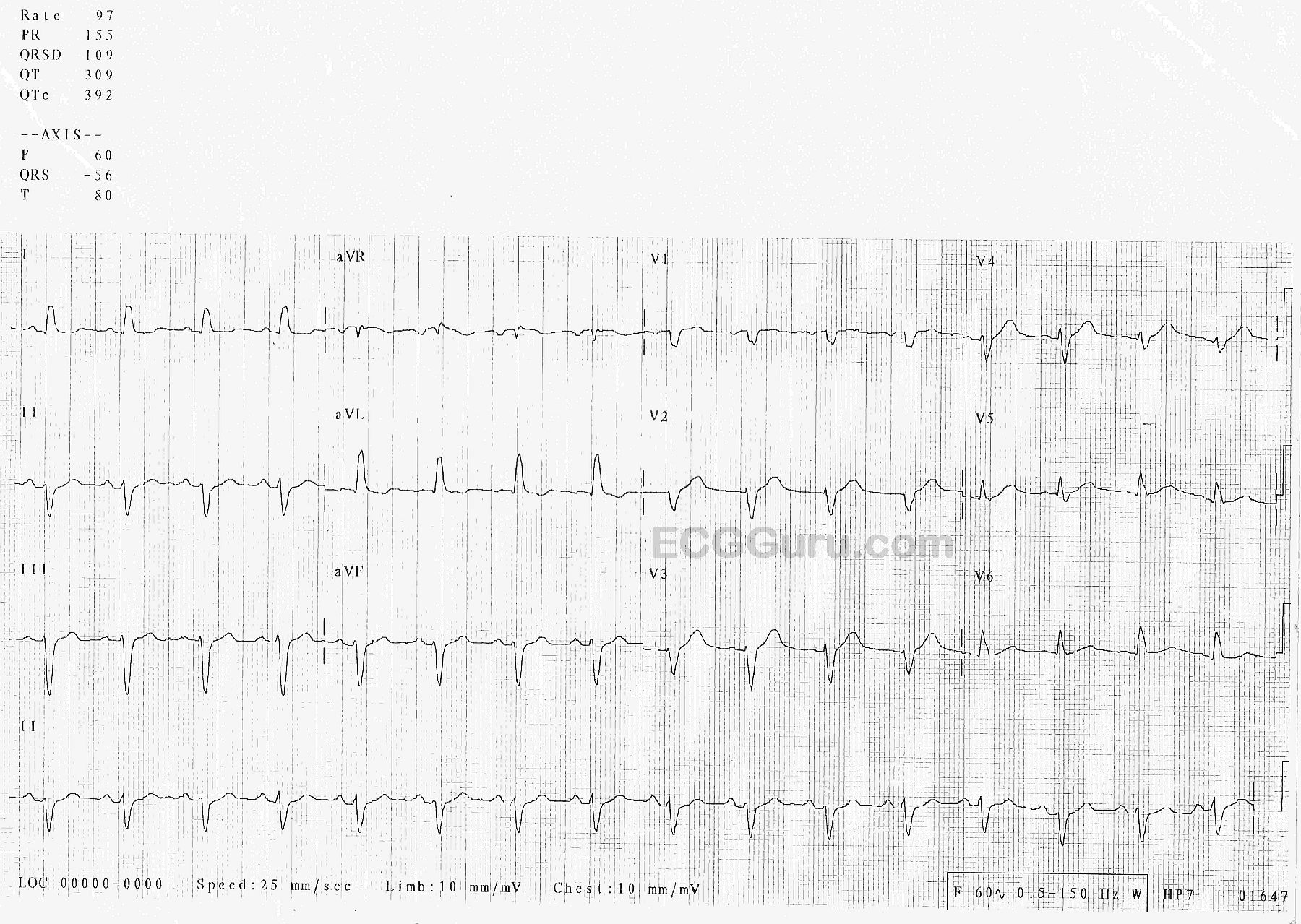
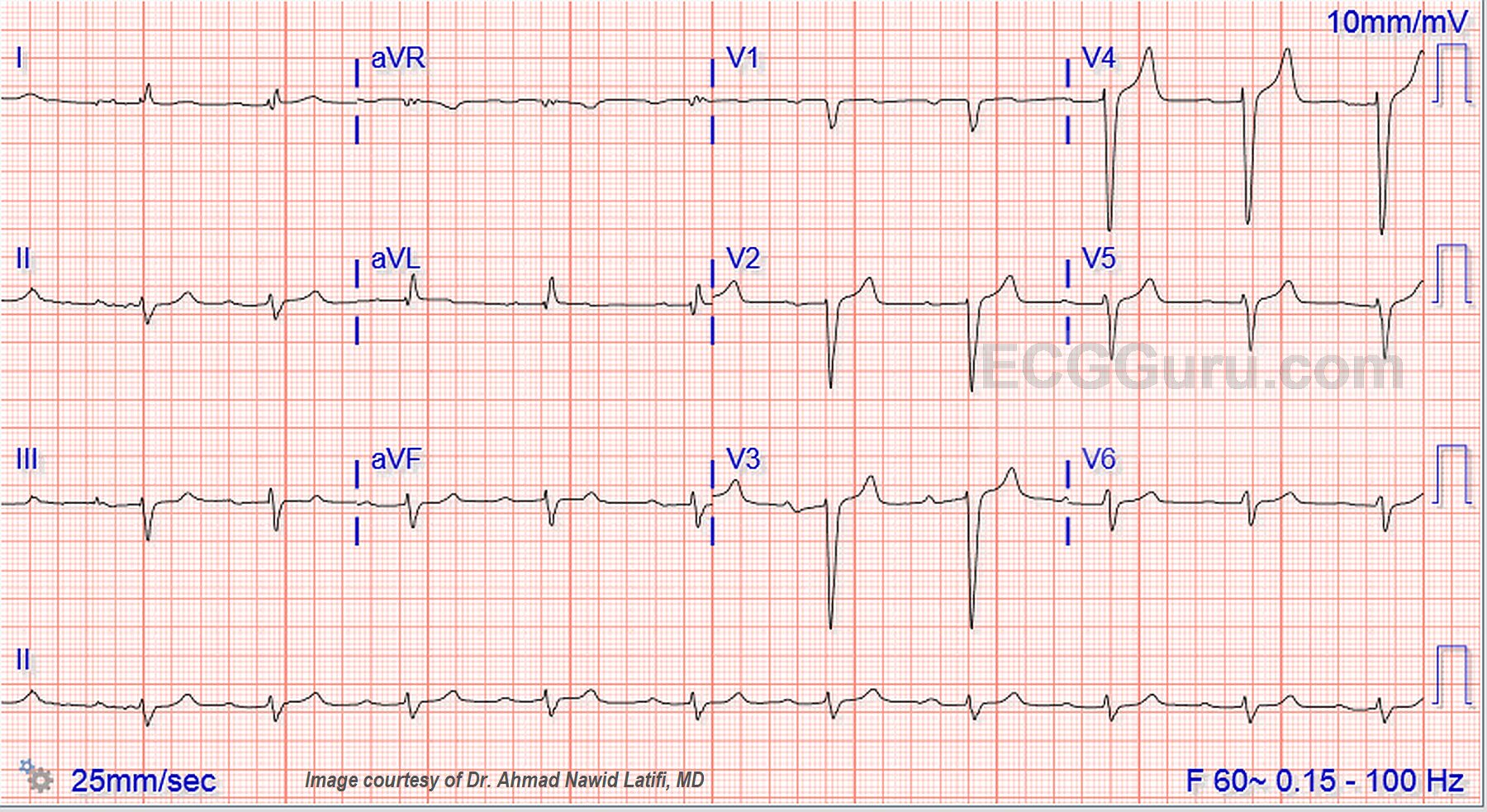
The Patient:This ECG was obtained from an elderly man who was suffering an exacerbation of congestive heart failure.He had a history of CHF and hypertension.We do not have other history available to us.
The ECG:The rhythm is sinus at 97 bpm (fast for this patient). It is regular with no ectopy.The PR interval is 155 ms (.15 seconds), and the P waves are upright in the inferior leads. The frontal plane QRS axis is -56 degrees – abnormally leftward.Notice that Leads II, III, and aVF are all negative.AVR is equiphasic – the axis travels perpendicular to the positive electrode of aVR, toward the patient’s left shoulder.The QRS duration is 111 ms (.11 sec.). This is very close to being wide enough for a diagnosis of left bundle branch block, and represents poor conduction throughout the ventricles. On the chest leads side, there is poor R wave progression. V1 through V4 look almost the same, small r and large S.
The ST segments are generally concave up, and the J points are at the baseline – no ST elevation or depression.There are no pathological Q waves, unless we count V1, which may have lost it’s Q wave as part of the general poor R wave progression.
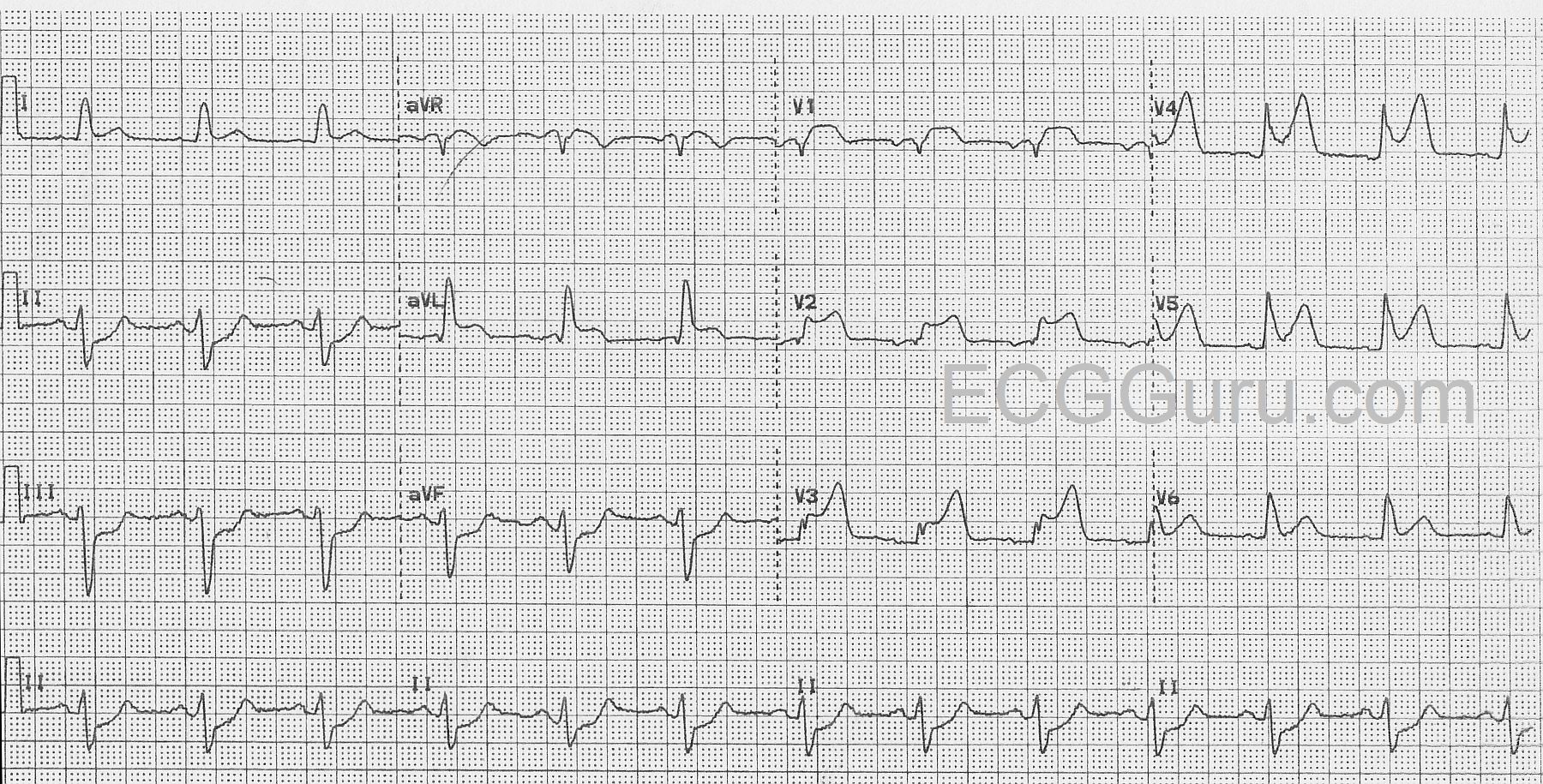
The Patient:An elderly man presents with chest pain, pallor, diaphoresis and weakness.
The ECG:The rhythm is normal sinus at a rate of about 76 bpm with normal intervals. The QRS complexes are wide at about .14 seconds (140 ms).There is ST segment elevation in all precordial leads, except for possibly V6.The shape of the ST segments in the anterior wall range from coved upward in a “frowning” shape (V1) to very straight (V5 and V6).There is also ST elevation in aVL with ST straightening in Lead I.There is ST depression in the inferior leads, II, III, and aVF.Lead II is equally biphasic while I and aVL are positive, indicating an axis that is shifted slightly to the left.With his symptoms and this alarming ECG, he was sent promptly to the cath lab.
Interpretation:The rather obvious ST-elevation M.I. is extensive, covering the entire anterior wall, and extending into the high and low lateral walls . This was confirmed in the cath lab, as the patient had an occlusion of the left anterior descending artery near the bifurcation of the circumflex.The wide QRS meets the criteria for left bundle branch block (wide QRS, negative QRS in V1 and positive QRS in V6 and Lead I).However, it doesn’t have the “look” of LBBB with the low-voltage seen in the anterior wall. After the offending artery was opened and stented, the wide complex became narrow and was considered to be an interventricular conduction delay that was due to the ischemia.The ST depression in the inferior wall is most likely reciprocal.
The Patient:This ECG was taken from a 73-year-old man with a history of heart failure with preserved ejection fraction, severe left ventricular hypertrophy, Type II diabetes, and stage 4 chronic kidney disease.He also suffered deep vein thrombosis and is on anticoagulation.He has a recent diagnosis of IgA myeloma.He presented with a complaint of nausea and vomiting and was found to have a worsening of acute kidney infection.There was suspicion of renal and cardiac amyloidosis, but the patient refused biopsy to confirm this.He was started on chemotherapy for multiple myeloma and will be followed as an outpatient.
The ECG:The rhythm is sinus at around 60 bpm, although the rate varies a little at the beginning of the strip.The QRS complex is wide at .12 seconds, or 120 ms., representing interventricular conductiondelay (IVCD).The PR interval is .32 seconds, or 320 ms. This constitutes first-degree AV block.There is left axis deviation in the frontal plane and poor R wave progression in the horizontal plane.
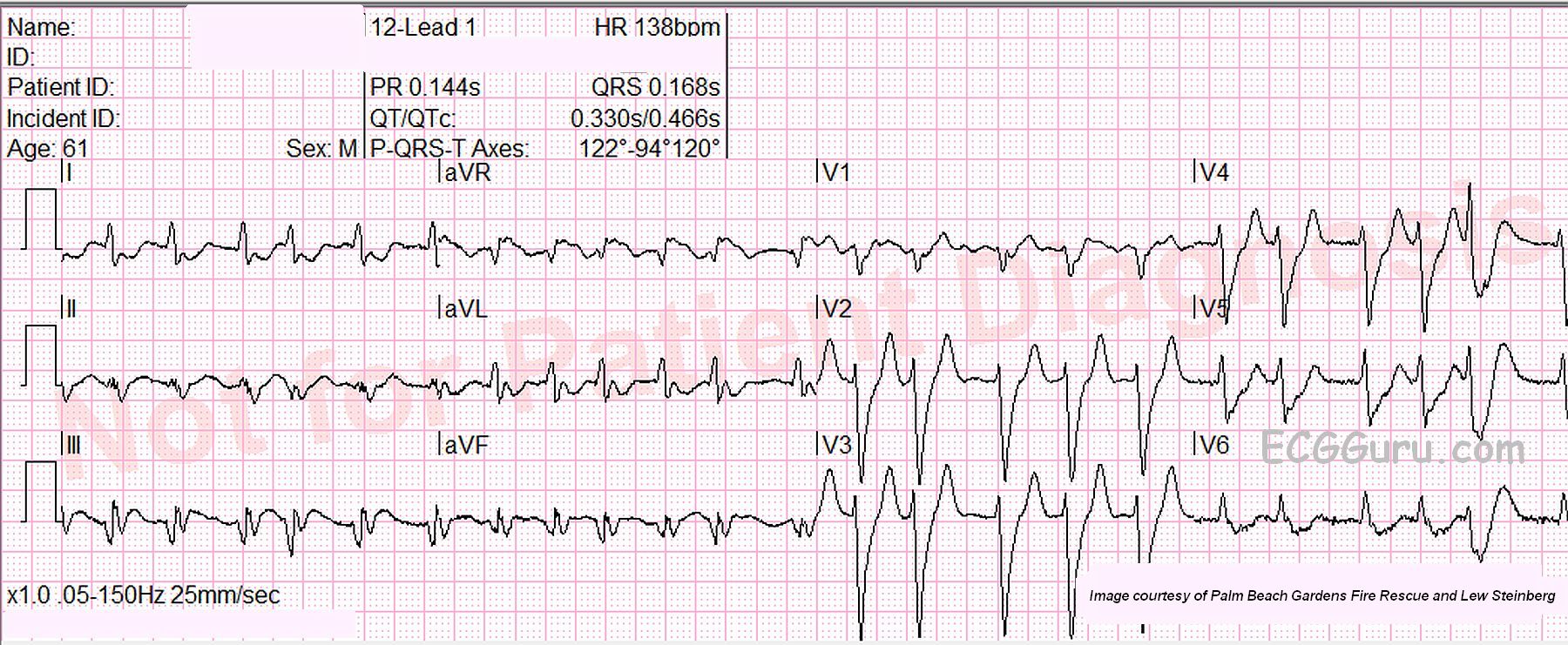
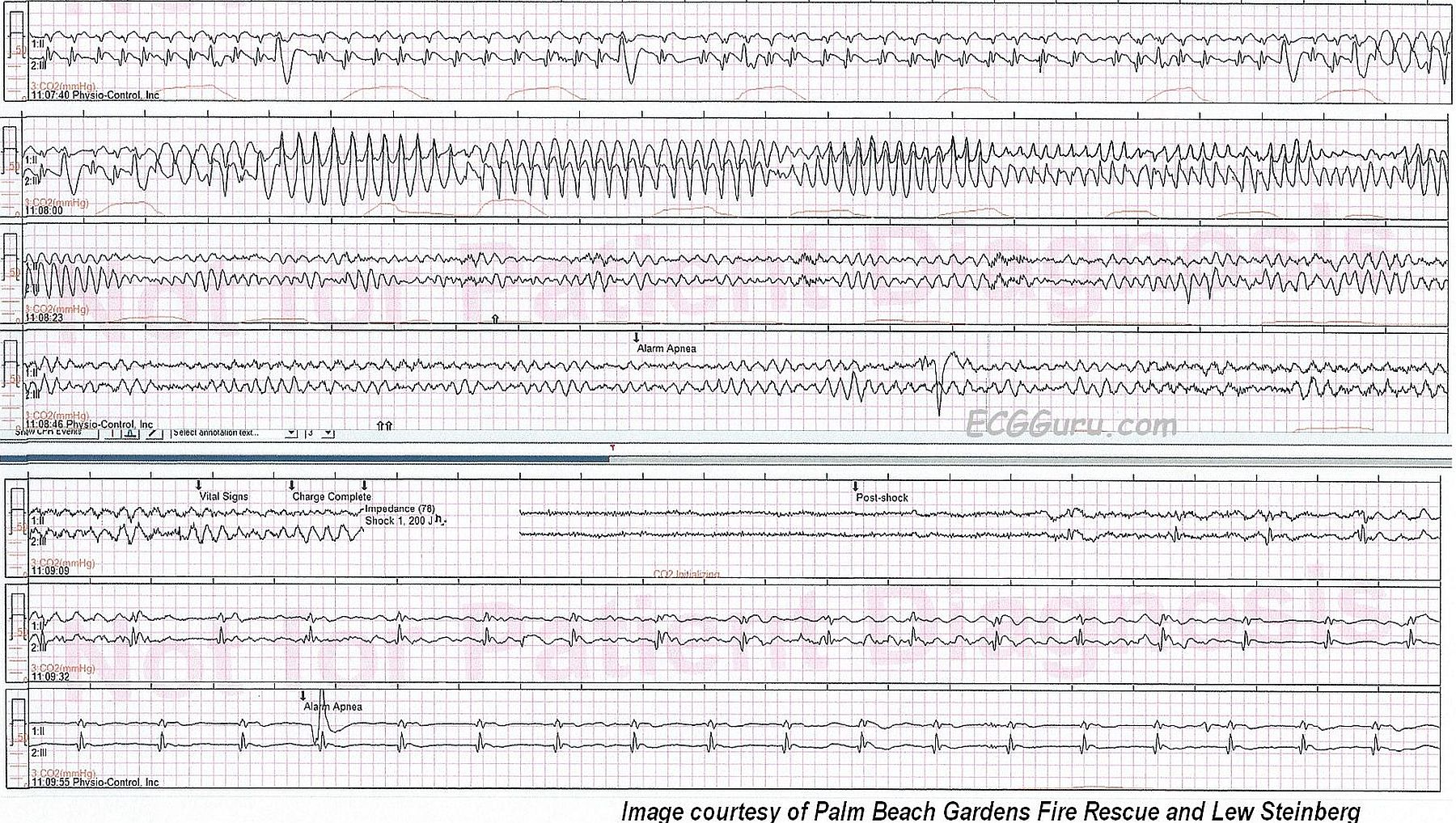
A paramedic crew responded to the office of a local physician. A 61-year-old male presented with a one-week history of chest pain and shortness of breath. He had a previously undiagnosed atrial fibrillation with rapid ventricular response and left bundle branch block, but was alert. Shortly after transport commenced, the patient became unresponsive with Torsades de Pointes, which rapidly degenerated into ventricular fibrillation. The paramedic placed pads and defibrillated within one minute. After two minutes of compressions, the patient had a fairly regular rhythm with return of spontaneous circulation. Transport time was short. On catheterization, the patient was found to have severe coronary artery disease, requiring coronary artery bypass graft surgery (CABG) A balloon pump was inserted in an attempt to strengthen him for surgery.
What is the rhythm? The 12-lead ECG presented here shows atrial fibrillation at a rate of 138 per minute.The rhythm is irregularly-irregular with no P waves.Since the patient had not yet been diagnosed with atrial fib, obviously no therapy had been initiated to control the rate. There is a PVC near the end of the strip.