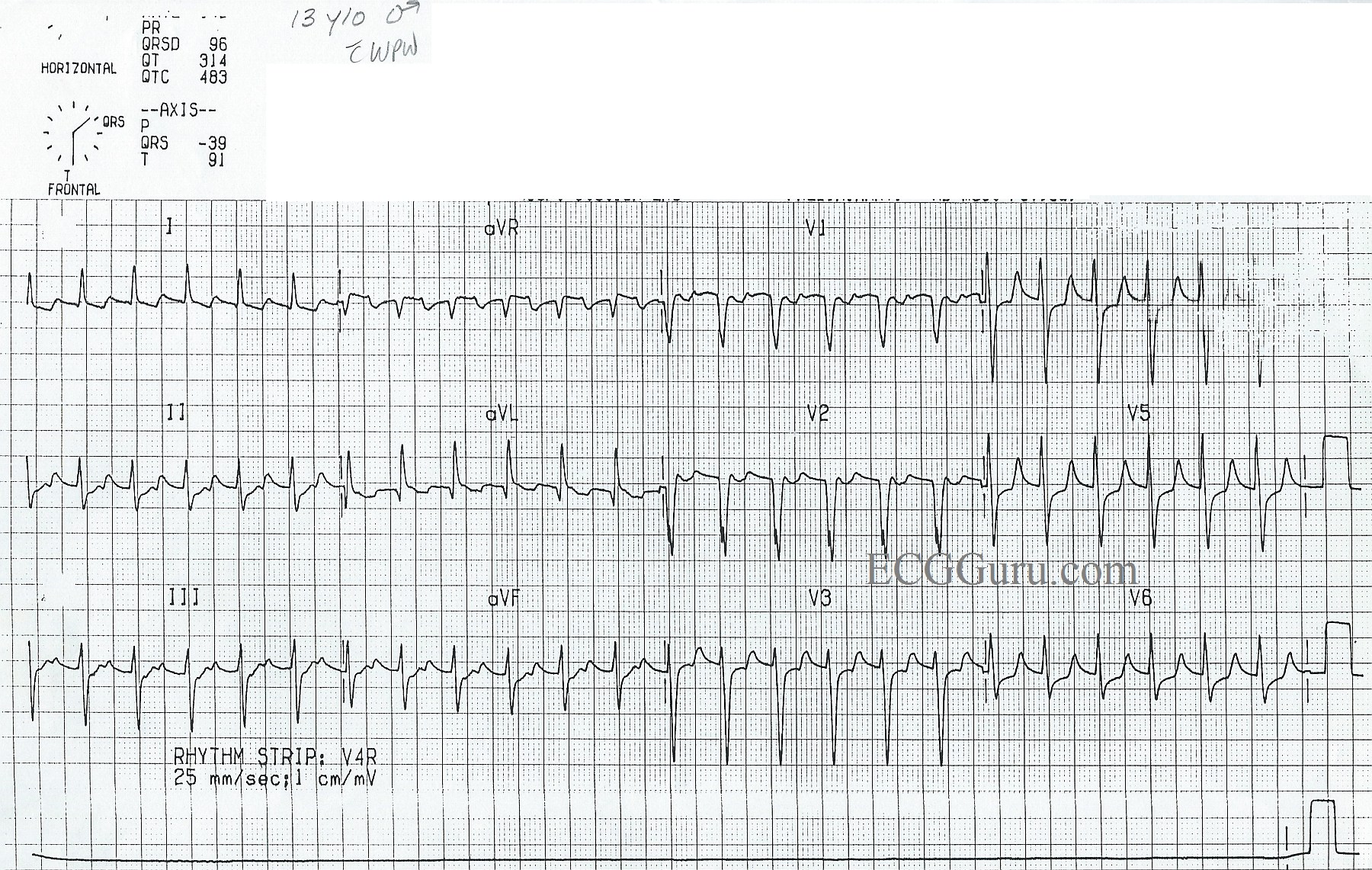
Here is a good example of an ECG showing the signs of Wolff-Parkinson-White syndrome during normal sinus rhythm. WPW is one of the “pre-excitation” syndromes caused by an accessory pathway between the atria and ventricles. Accessory pathways can bypass the AV node. These conduction pathways can conduct anterograde (forward toward the ventricles), retrograde (away from the ventricles), most commonly, in both directions. When the accessory pathway conducts in an anterograde fashion, it causes pre-excitation of the ventricles. See Illustration.
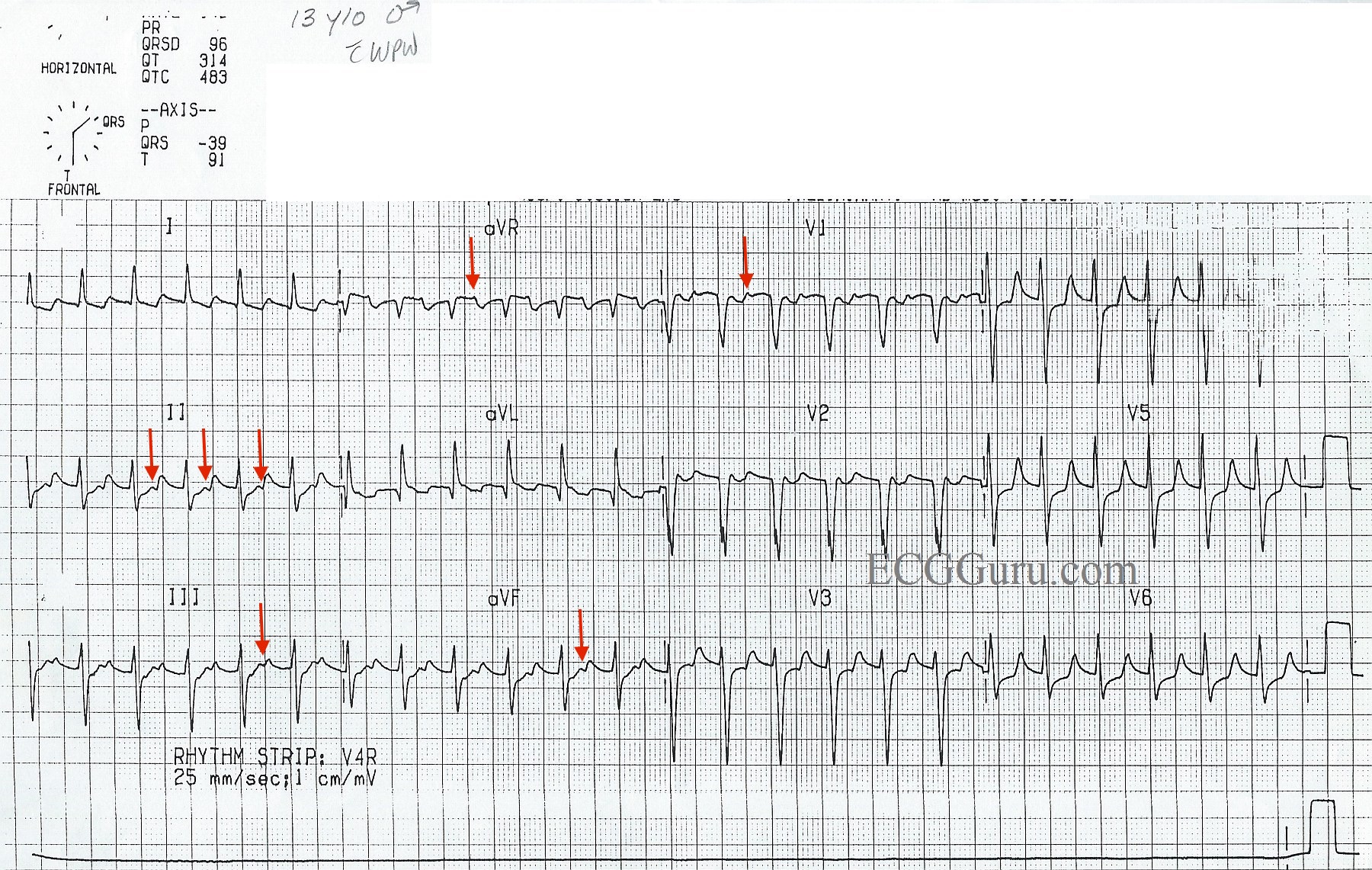
Wolff-Parkinson-White syndrome is caused by an accessory pathway called the Bundle of Kent, which can occur on either the left or the right side of the heart. The ECG sign of the pre-excitation of the ventricles in WPW is a DELTA WAVE. The delta wave is seen in normal sinus rates when the accessory pathway conducts anterograde, pre-exciting the ventricles. The delta wave arises at the end of the P wave, eliminating the PR segment in some leads. In this ECG, the delta waves can best be seen in Leads I, II, aVR, and aVL, as well as in V1, V2, and V3.
People with WPW are prone to bouts of supraventricular tachycardia, called AV reentrant tachycardia (AVRT). A circular pathway can form between the normal AV pathways and the accessory pathway, causing an impulse to depolarize the ventricles and return to the atria in a rapidly repeating cycle, causing a paroxysmal supraventricular tachycardia. The delta waves will disappear as they become part of the reentrant cycle.
Tachyarrhythmias can also form when impulses from atrial flutter or atrial fibrillation rapidly enter the ventricles through the accessory pathway without the filtering effect of the AV node. The extremely rapid rates produced in these situations can quickly lead to deterioration and ventricular fibrillation.
For more information on WPW ECG signs, we recommend Life In The Fast Lane.