
Submitted by Dawn on Wed, 06/03/2015 - 21:25
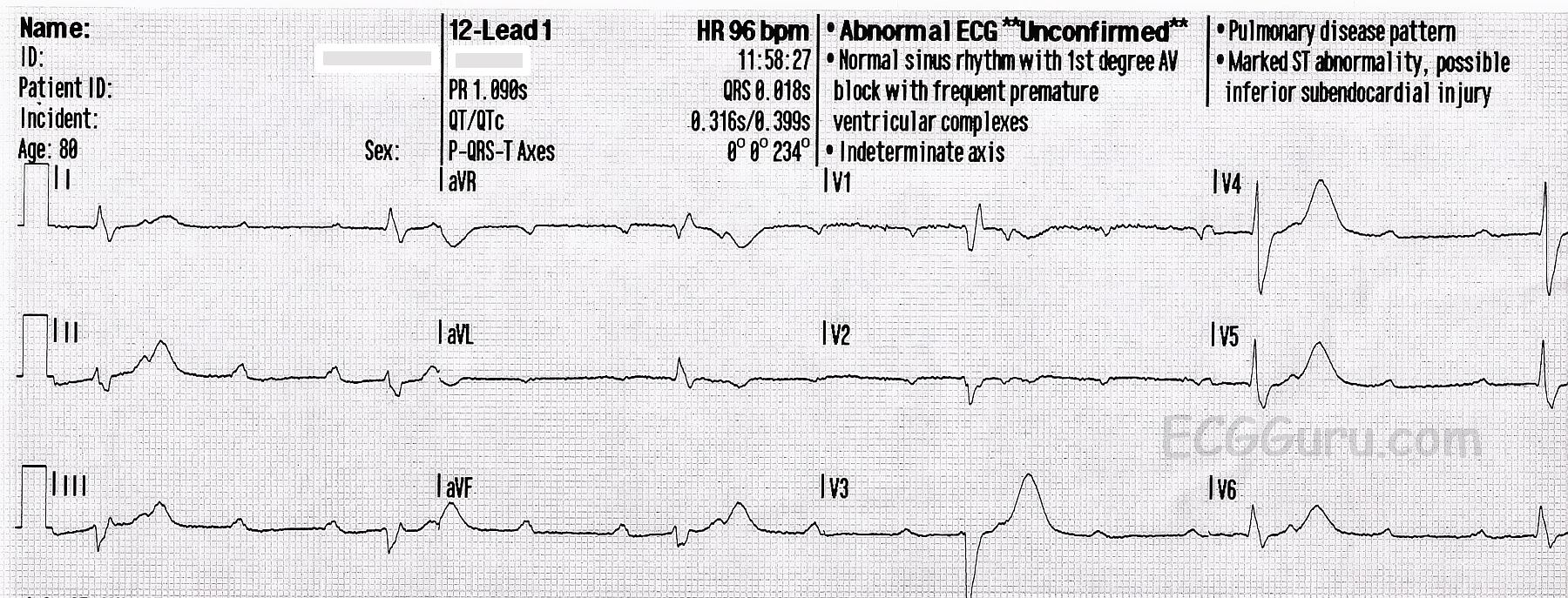
This ECG shows a second-degree AV block, Mobitz Type II. It is also called “high grade AV block” because there is a 3:1 ratio of P waves to QRS complexes and a resulting slow rate.
Right bundle branch block and left anterior fascicular block are also present, as is common with Type II blocks. The underlying rhythm is sinus. Second-degree AVB, Type II, usually represents an intermittent tri-fascicular block: often right bundle branch block and left anterior fascicular block (hemiblock) are present, and the left posterior fascicle develops an intermittent block. During times of tri-fascicular block, the P waves are not conducted. When the posterior fascicle is conducting, a QRS occurs.
A differential diagnosis for this ECG is complete heart block with ventricular escape rhythm. A longer strip would be needed to see the P waves eventually dissociate from the QRSs, if they are going to do so. Clinically, there is really little difference in the treatment of a high-grade "second degree" block and a "third degree" block. Both are treated with emergency support of the slow rate, as needed, and then a permanent implanted pacemaker.
It is notable that, in this case, the interpretation given by the machine is completely incorrect, even including the intervals. This is not common, but does occur. The machine's interpretation should be considered, but not followed blindly.
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Mobitz 2 with 3:1 AV Conduction (and RBBB/LAHB)
Ken Grauer, MD www.kg-ekgpress.com [email protected]