
Submitted by Dawn on Tue, 09/16/2014 - 14:26
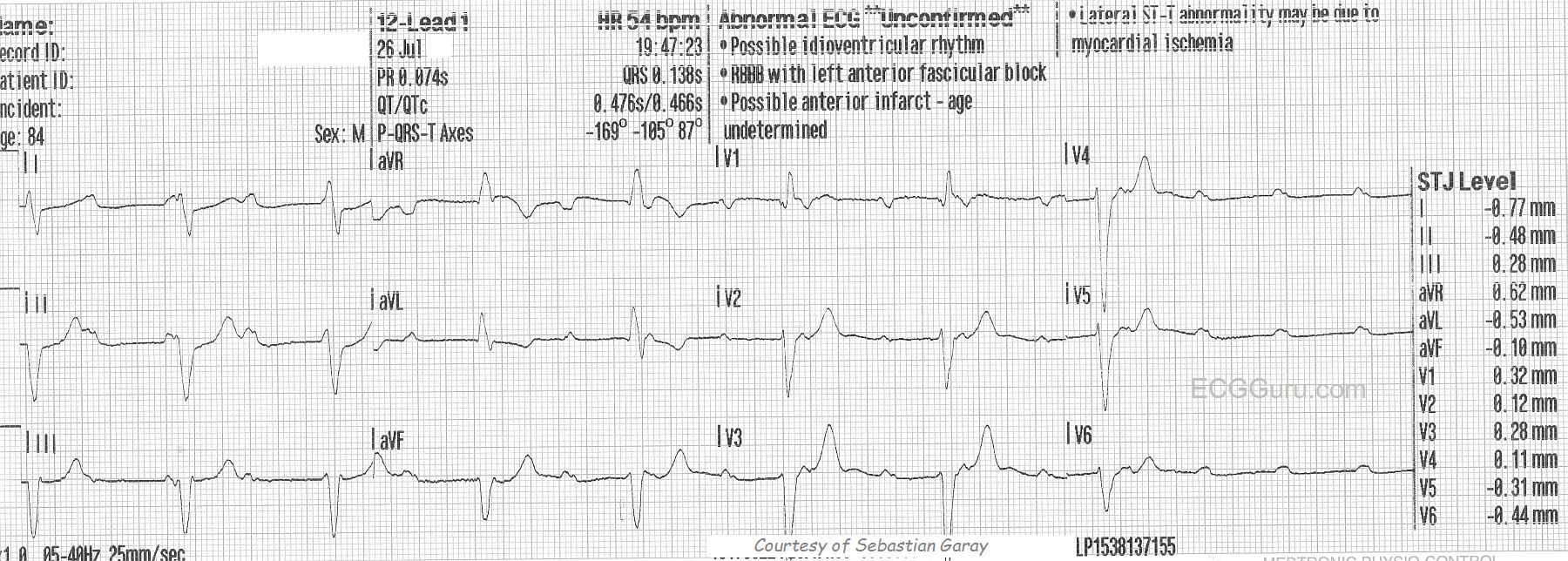
This ECG is from an 84-year-old man who experienced dizziness and a fall. He was not injured in the fall. In this ECG, we can clearly see regular P waves at about 110 per minute. We also see wide QRS complexes at about 52 per minute. There is AV dissociation - there are no regular PR intervals, or even progressively-prolonging PR intervals. The atrial and the ventricles are beating to separate rhythms. What is interesting about this rhythm is the origin of the escape rhythm. The wide complex suggests a ventricular focus and the rate suggests supraventricular origin. Near the end of the ECG, the escape rhythm either fails or slows significantly. To see the next 12-lead ECG for this patient, go to this LINK.
The second ECG makes it more clear that this is an idioventricular escape rhythm, but the morphology of the QRS complexes suggested that, even in the first ECG when the rate was faster. There are several clues that this is probably ventricular, including a very "backward" axis with aVR being upright and II, III, and aVF all being negative. Also, V6 is negative, and there is nearly precordial concordance: all except V1 are negative. The morphology of the QRS does not fit a diagnosis of either left bundle branch block OR right bundle branch block. The evidence points to a ventricular origin for this escape rhythm, and the patient quickly goes on to slow down severely. Ventricular escape rhythm strongly suggests a sub-Hisian location for the block, and they tend to be more life-threatening than supra-Hisian blocks.
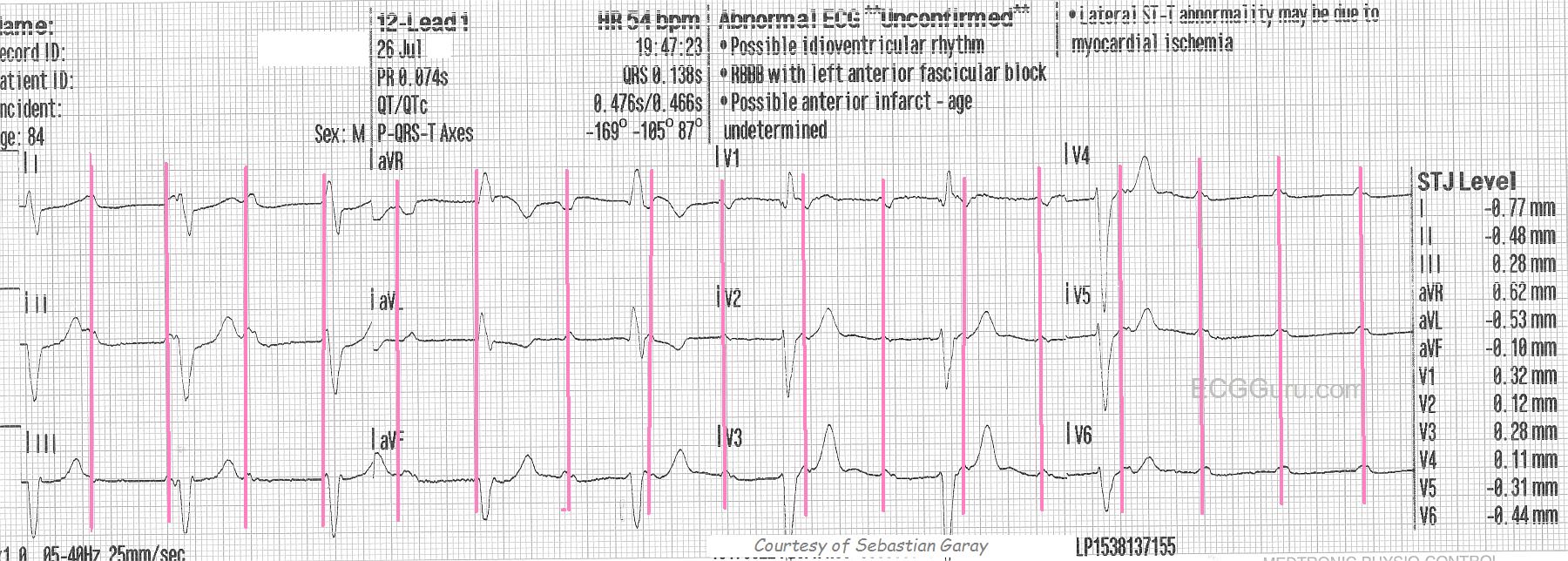
The take-home clinical lesson here is to BE PREPARED for worsening of the rate whenever AV block is present, especially high-grade AV block or sub-Hisian block. This ECG is a very good one for teaching students to "march out" P waves, and find "hidden" P waves. We have included a marked copy of this ECG to indicate those P waves.
Thanks to Sebastian Garay for donating these ECGs.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Complete AV Block with Ventricular Standstill
NOTE: We review the Basics of AV Block in a 50-minute Video (GO TO — www.avblockecg.com ).
Ken Grauer, MD www.kg-ekgpress.com [email protected]