
Submitted by Dawn on Sat, 09/21/2013 - 22:45
This week's ECG for your collection was kindly donated by Dr. Stasinos Theodorou, interventional cardiologist with the Limassol Cardiology Practice in Cyprus. It offers a wonderful teaching opportunity, and illustrates how valuable an ECG can be in locating a lesion during an M.I. Dr. Theodorou previously posted this ECG and the angiograms from the same patient on FaceBook, and he has offered them to the users of the ECG Guru website free of copyright.
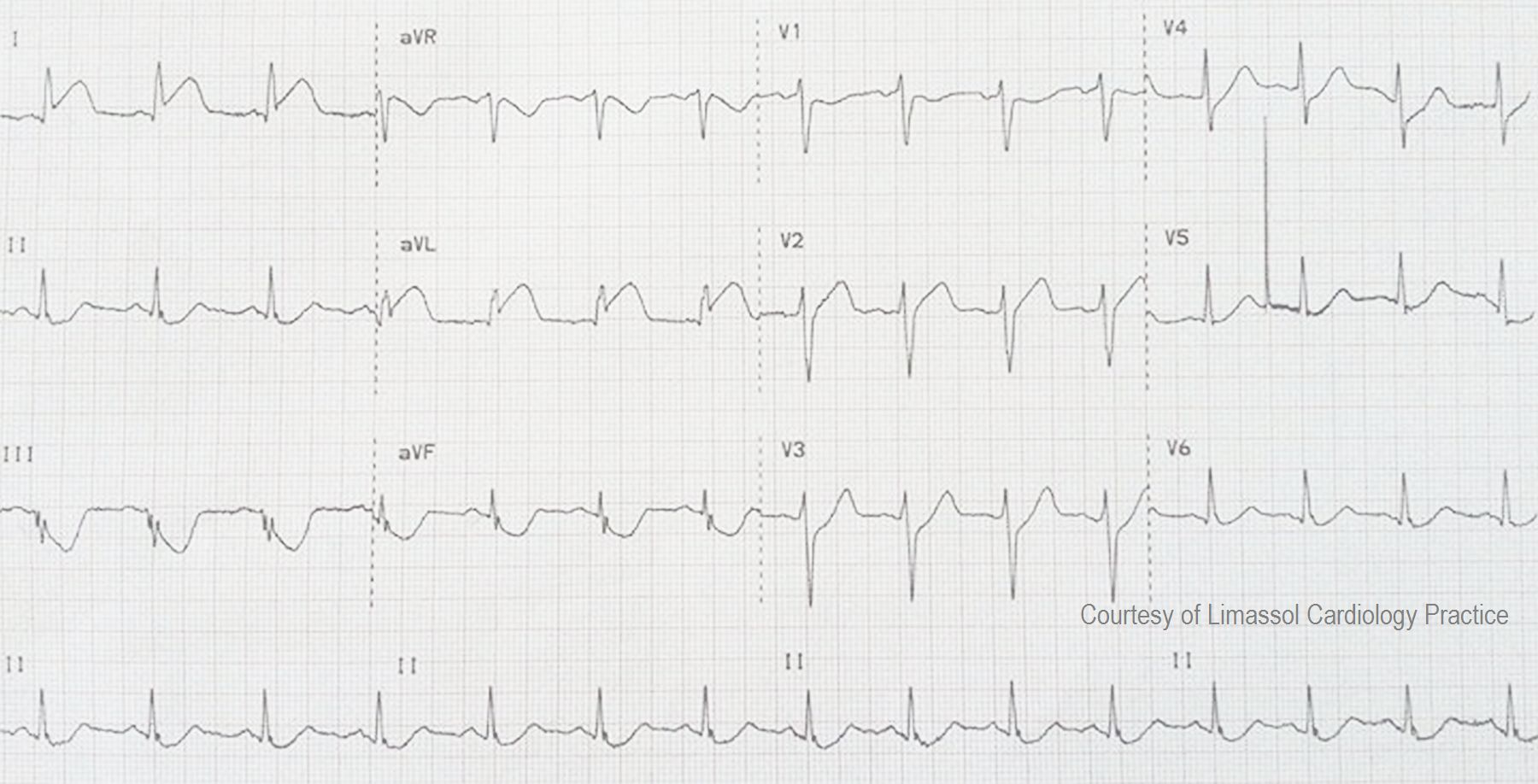
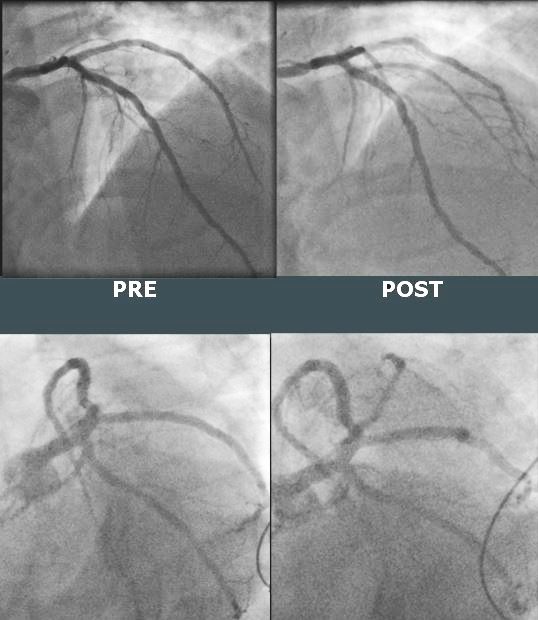
Dr. Theodorou reports that the culprit lesion in this M.I. was initially very difficult to find on angiogram. In this case the culprit was an ostially occluded second diagonal artery which, due to the anatomy, was almost impossible to spot from the initial diagnostic images. There was no "stump" because the occlusion was in the ostium - the beginning of the artery. The patient also had a significant right coronary artery lesion, but it was not the cause of the M.I. because the RCA perfuses the right ventricle and inferior/posterior wall of the left ventricle. The ST elevation in this ECG is in I and aVL - the area of the high lateral wall. Because the ECG appeared to be inconsistent with the angiogram, Dr. Theodorou obtained further projections, allowing him to identify and treat the offending lesion. This illustrates the importance of the ECG in locating coronary artery lesions, even in this age of high technology and cath labs. The interventional cardiologist's proficiency in ECG interpretation enabled him to find this "invisible" lesion.
We are grateful to Dr. Theodorou for sharing this valuable learning experience with us. You can find more from Dr. Theodorou on his website, FaceBook page, and here, on our "Ask the Expert" page.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
How to Recognize Acute Occlusion of 1st or 2nd LAD Diagonal
Great teaching case — with our gratitude to Dr. Stasinos Theodorou for posting the ECG and cath films on the ECG Guru (and for allowing us copyright-free use of this material! ).
Ken Grauer, MD www.kg-ekgpress.com [email protected]