
Submitted by Dawn on Fri, 11/18/2016 - 20:30
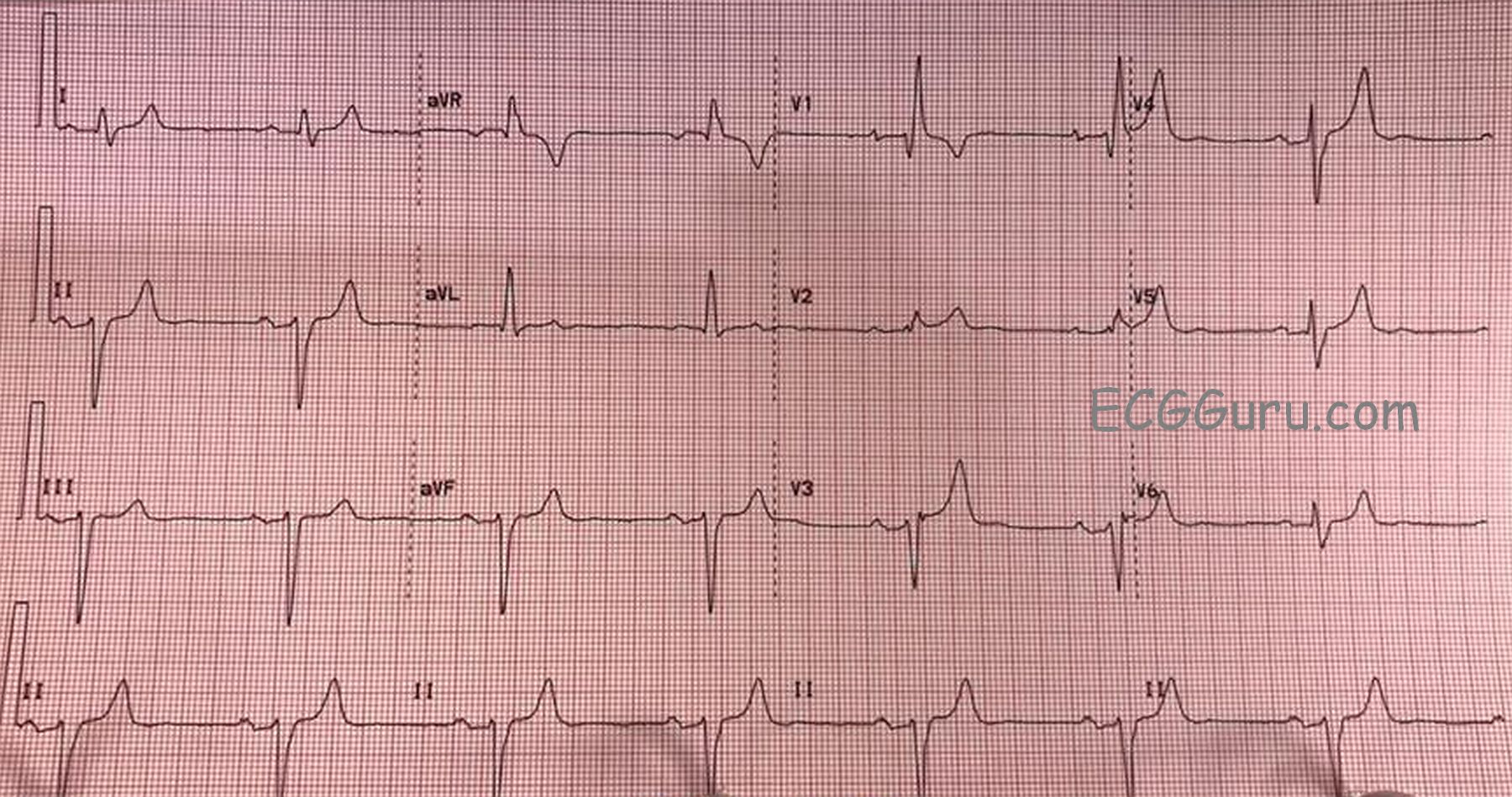
Today’s ECG is from a 75 year old man who has been experiencing syncope.
Examination of the ECG shows a sinus bradycardia at just under 40 bpm. There is a first-degree AV block, with a PR interval of about .28 seconds (280 ms). There is a right bundle branch block. The ECG criteria for right bundle branch block are: supraventricular rhythm, wide QRS (120 ms in this case), rSR’ pattern in V1, and a small, wide S wave in Leads I and V6. There is actually a “terminal delay”, or extra wave at the end of each QRS complex, reflecting late repolarization of the right ventricle.
This ECG also shows a left anterior fascicular block, also called left anterior hemiblock. The left bundle branch usually has two main branches, the anterior-superior and the posterior-inferior. ECG criteria for left anterior fascicular block are: left axis deviation with a small r wave in Lead III and a small q waves with tall R waves in Leads I and aVL. There is also a prolonged R wave peak time (> 45 ms) in aVL. There is usually a slightly prolonged QRS, but in this case, there is widening of the QRS due to the RBBB. Because the right bundle branch is blocked, and one fascicle of the left bundle is blocked, the patient is said to have a “bifascicular block”. Only one fascicle remains available for conduction from the atria to the ventricles.
We have no information about what caused the conduction block in these two fascicles, but should the third fascicle fail, the patient will be in a complete AV block. An AV block at the level of the bundle branches will result in an idioventricular escape rhythm – wide QRS complexes with very slow rates – which is a low-output rhythm.
This patient has also had syncope, which was determined to be related to his bradycardia. He had an AV sequential pacemaker implanted and did well.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Is There "Tri-Fascicular" Block?
Interesting tracing which brings up some additional points/questions to the explanation provided by Dawn. As noted — there is a long PR interval ( = 1st-Degree AV Block) + RBBB + LAHB ( = Left Anterior HemiBlock). In the past, this combination of conduction defects would be call “Tri-Fascicular Block”, on the thinking that the long PR interval implied conduction delay in the third (and only remaining) conduction fascicle. The problem with this approach is that we have no idea from the surface ECG if the cause of the prolonged PR interval is due to conduction delay prior to arrival at the AV node — or after leaving the AV node (as a result of impaired conduction in the remaining posterior hemifascicle). Because there are only rare instances in which accurate determination of true “Tri-Fascicular Block” can be made from the surface ECG (ie, baseline RBBB with alternating LAHB and LPHB from one beat to the next) — use of this term is best avoided. Instead, it is recommended to simply describe what is seen (ie, 1st-Degree AV Block + RBBB + LAHB), as was done in this case. Regardless of whether all 3 fascicles of the conduction system are impaired — justification for a pacemaker is clear in this case (ie, an older patient with recurrent syncope who manifests marked bradycardia with the conduction defects we see).
Otherwise — T waves are obviously peaked and pointed in many leads on this tracing. This is most probably due to either: i) Hyperkalemia; or ii) Ischemia that may be recent or acute. Given symmetric upslope and downslope of ascending and descending limbs of those T waves that are tall and peaked — my initial clinical move would be to determine the serum K+ value. If not elevated — then this T wave appearance points to recent ischemia that may be the cause of the conduction problems we see. Finally — the ST-T wave appearance in lead V2 is definitely abnormal. One just should not see the ST elevation we see in this lead. This could be the result of hyperkalemia — but if serum K+ is normal, recent infarction should be suspected …
Ken Grauer, MD www.kg-ekgpress.com [email protected]
Interest in reading ECG
Hello
I am a RN who over 10 years ago worked in a CCU and cardiology has been my favorite subject, yet. I am a novice at basic interpretation of rhythms, blocks, st elevation/depressed, etc. This is a great site to sharpen my skills on axis deviation, BBB, Left vs. right and fascicular.
If you don not use it, you lose it.
Great analysis/diagnostic explanations
Thank You
Donna B. RN
Hi, Donna,
Thanks so much for your comment, and sorry for the delay getting back to you. We are so glad you enjoy the ECG Guru. Please let us know if you have any questions or suggestions for us.
Donna Bailey