
Submitted by Dawn on Sun, 12/15/2013 - 20:16
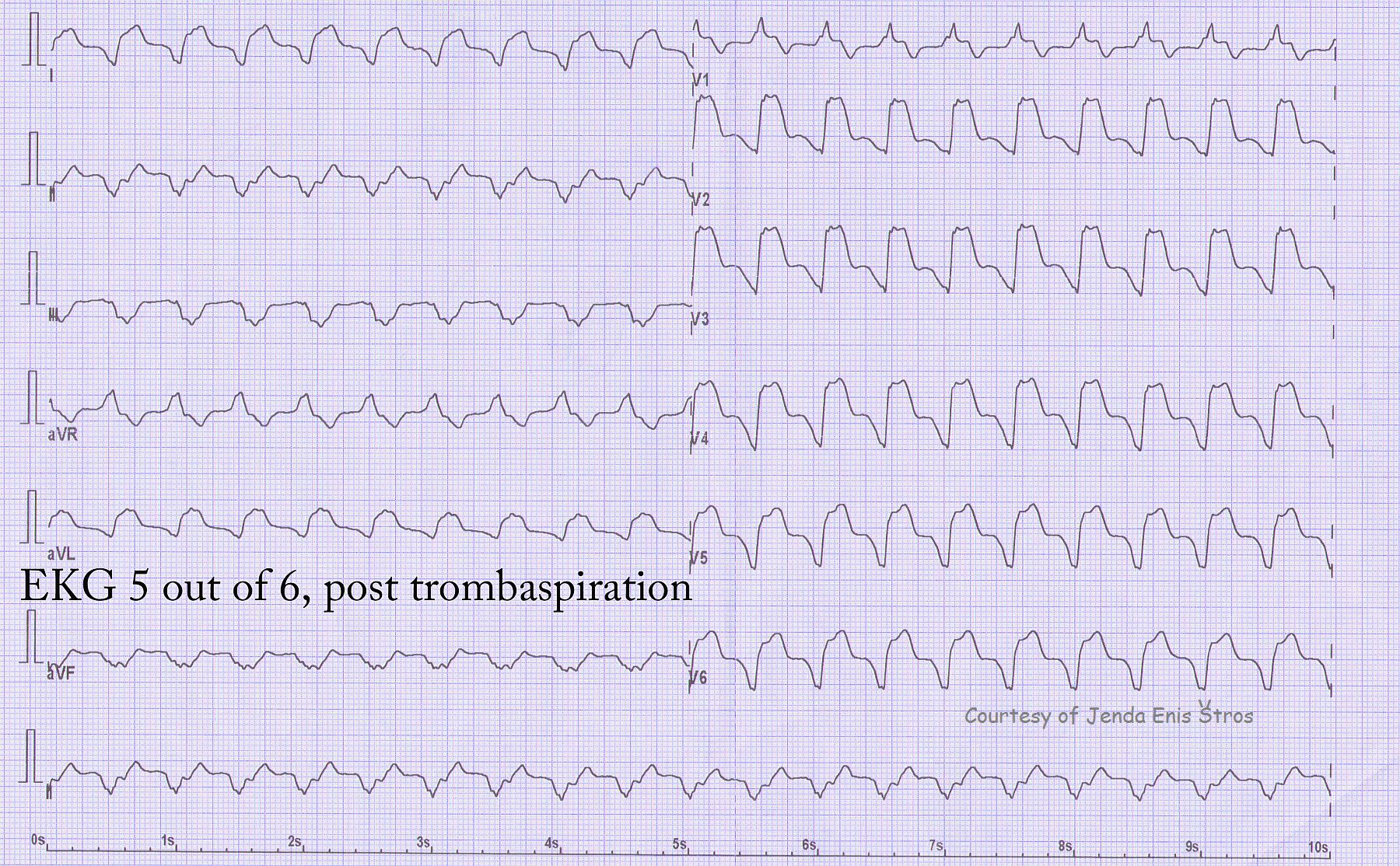
Continuing our series from the patient with acute AWMI, donated by Jenda Enis Štros, a new dysrhythmia has appeared. The patient was taken to the cath lab, and a thrombus was removed from the stent. We now see a wide-complex tachycardia. The morphology (shape and configuration) of the QRS has changed considerably from the previous ECGs, so we know this is idioventricular in origin. There are many other clues, but some major ones are: the QRS is very wide, there is no associated P wave, all the precordial leads except V1 are negative (precordial concordance), V6 is negative, and the axis is away from II, III, and aVF and toward aVR (aVR is upright).
Because the rate is about 125/min., this could be called ventricular tachycardia (V Tach) or accelerated idioventricular rhythm (AIVR). The important fact here is that this rhythm was transitory and the patient remained stable. Reperfusion dysrhythmias are not uncommon, and the patient is treated as indicated by the clinical condition.
Here are links to all six ECGs in this series:
http://www.ecgguru.com/ecg/teaching-series-1113-ecg-1-6-acute-anterior-wall-mi
http://www.ecgguru.com/ecg/teaching-series-1113-ecg-2-6-acute-anterior-wall-mi
http://www.ecgguru.com/ecg/teaching-series-1113-ecg-3-6-acute-anterior-wall-mi
http://www.ecgguru.com/ecg/teaching-series-1113-ecg-4-6-acute-anterior-wall-mi
http://www.ecgguru.com/ecg/teaching-series-1113-ecg-5-6-acute-anterior-wall-mi
http://www.ecgguru.com/ecg/teaching-series-1113-ecg-6-6-acute-anterior-wall-mi
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.