
Submitted by Dawn on Sat, 12/22/2012 - 13:41
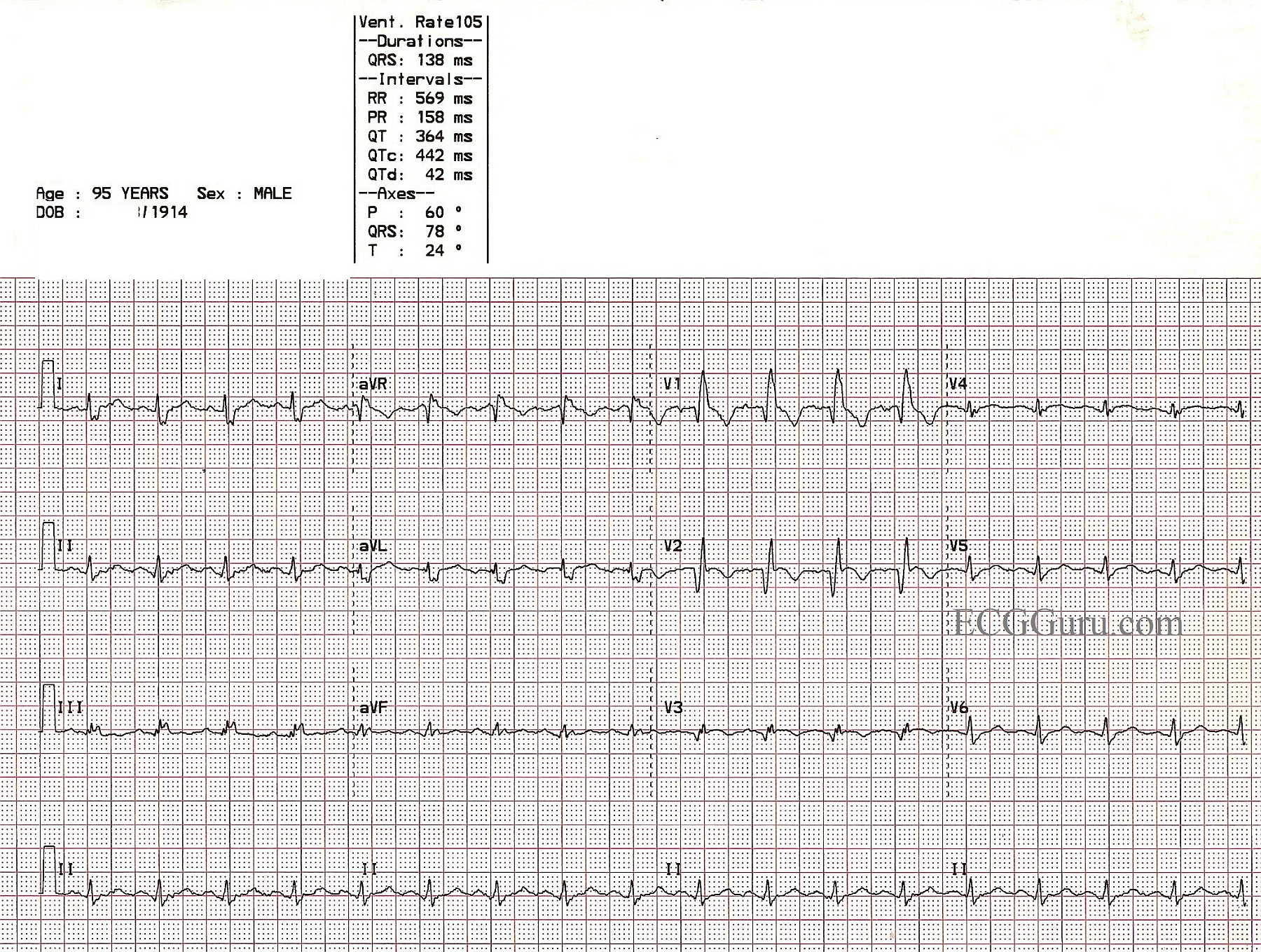
This example of previous anterior wall M.I. with right bundle branch block is from a 95-year-old man. He survived an anterior-septal M.I. caused by an occlusion of the left anterior descending branch of the LCA. The septum was involved in the damaged area, and the patient was left with a right bundle branch block. The pathological Q waves in Leads V1 through V3 show the location of permanent damage, or necrosis.
In this case, the usual rSR' pattern of right bundle branch block is replaced by qR, indicating loss of the initial r wave due to the M.I.
Review of RBBB criteria: wide QRS, rSR' pattern in V1, and Rs with a slurred s wave in I and V6. These criteria must be present in a SUPRAVENTRICULAR rhythm to diagnose RBBB.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
RBBB with Antero-Septal MI - of UNCERTAIN Age
Great teaching example by Dawn of previous anteroseptal MI plus RBBB in this 90yo man whose history is known. The only point I'd add to Dawn's insightful description is that IF you were given this ECG without the benefit of any past history (and with no prior ECG for comparison) - it would not be possible to "date" the infarction. As noted - the deep and wide Q waves in V1-to-V3 indicate previous infarction. However, ST segments remain coved and even slightly elevated in V2,V3 - which could signal recent infarction or reinfarction of new anterior (on top of previous anterior) damage.
Ken Grauer, MD www.kg-ekgpress.com [email protected]