
Submitted by Dawn on Tue, 11/12/2013 - 14:03
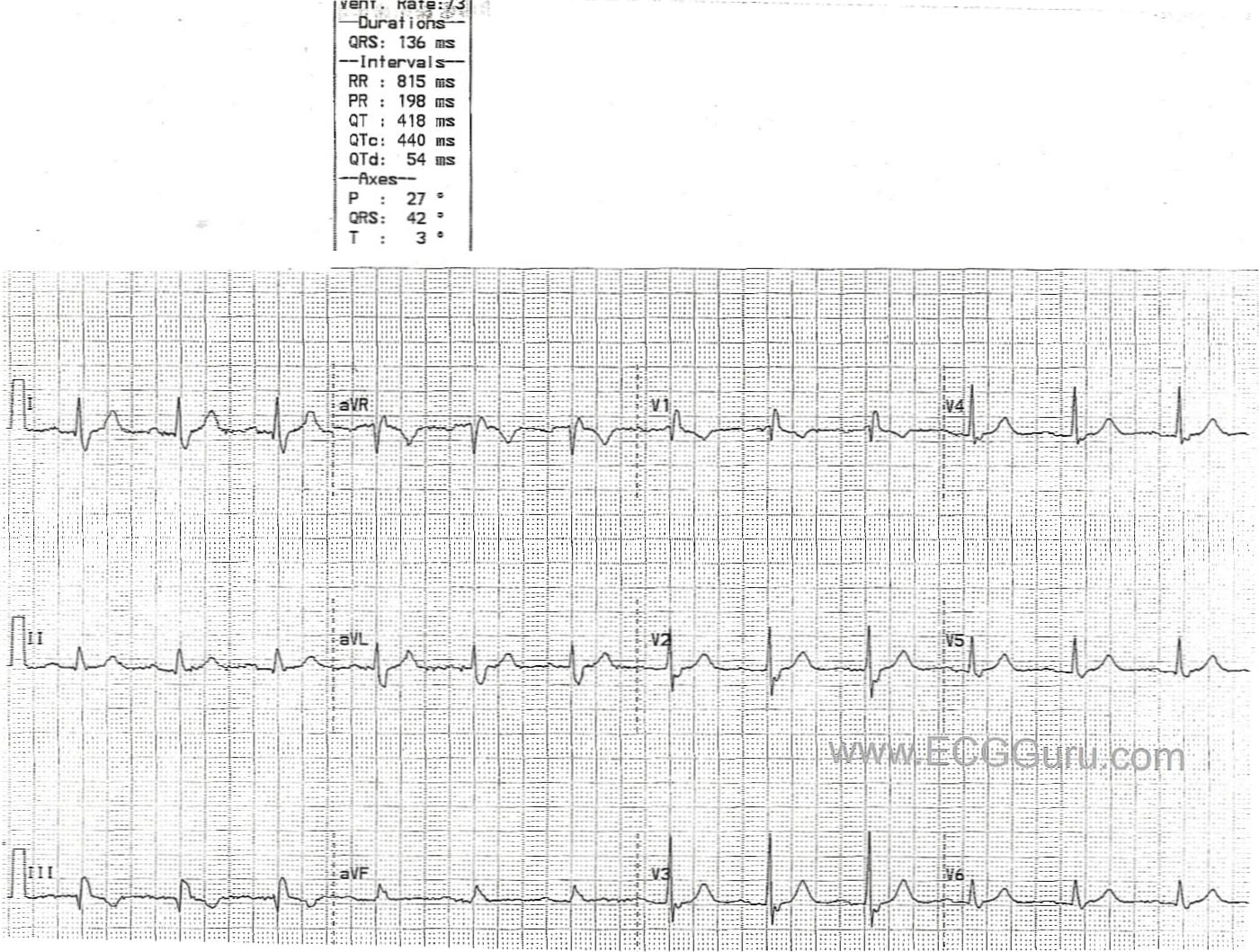
This ECG shows a normal sinus rhythm at 73/min. and a right bundle branch block. The diagnostic characteristics of RBBB are: wide QRS (greater than .12 sec.), supraventricular rhythm (in this case NSR), and an rSR' pattern in V1 with a small, wide S wave in Leads I and V6. The R' and small s waves represent the right ventricle depolarizing slightly AFTER the left ventricle. In fact, in RBBB, each lead should look pretty normal at first, with a terminal right ventricular depolarization wave added to each QRS complex. This is because the left ventricle depolalrizes normally. In this patient, R waves progress fairly soon in the precordial leads (V1 through V2). It is not known in this case if it is due to poor electrode placement or patient causes.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
ECG Diagnosis of RBBB
Good teaching example of RBBB posted by Dawn this week. I'd make the following teaching points regarding this tracing and ECG diagnosis of RBBB in general:
Ken Grauer, MD www.kg-ekgpress.com [email protected]