
Submitted by Dawn on Wed, 01/29/2014 - 23:05
Do you need a good example of normal precordial R wave progression for your collection? It is important to teach your students what "normal" looks like, as a reference for the abnormal ECGs you will teach them later.
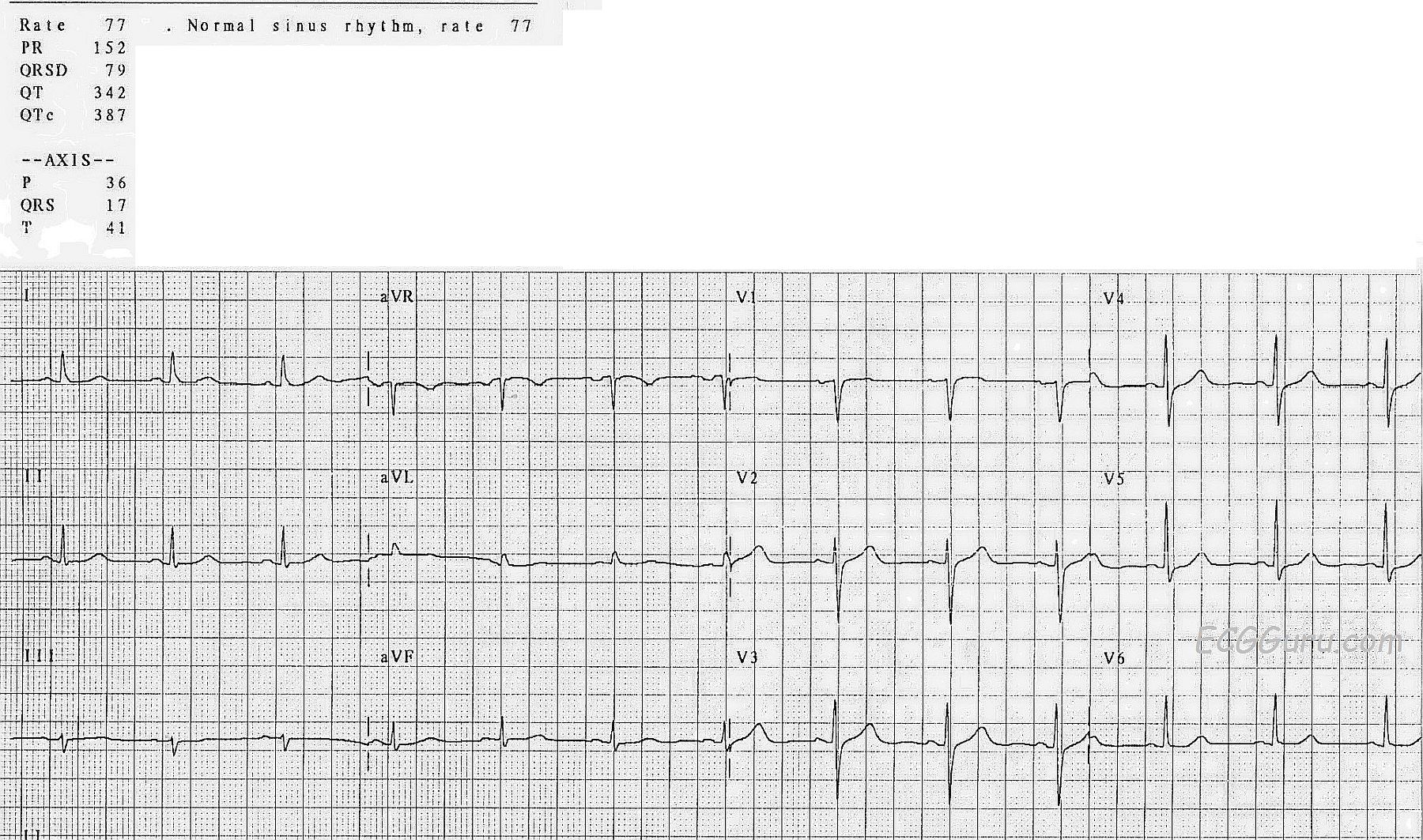
This 3-channel 12-lead ECG offers a normal frontal plane axis, as evidenced by Lead II having the tallest R wave of all the limb leads. It also demonstrates a normal "Z" axis. That is, the direction of depolarization on the horizontal plane is normal. This is seen in the progression of the QRS complexes from a negative V1 to a positive V6. Each of the chest leads should have an R wave. V1 normally has a small R wave, and a deeper S wave. The R wave reflects the depolarization of the septum, which flows TOWARD the V1 electrode. The S wave reflects the ventricles depolarizing, dominated by the left ventricle, which depolarizes AWAY from V1.
V6 will be all or nearly all positive, reflecting that the same heart is depolarizing TOWARD the V6 electrode, located in the 5th ICS in the mid-axillary line. When we evaluate the leads V2 through V5, we should see an orderly progression between the negative V1 and the positive V6. When viewed as an R-S ratio, we could say the R waves are becoming larger and the S waves smaller as we progress across the chest from right to left. Other factors, however, will affect the overall size of the QRS, such as the size and contents of the chest, and how close the electrode is to the heart. For that reason, the overall amplitude of V2 and V3 is usually larger, given their close proximity to the heart. V6 is smaller overall than V5 because it is farther from the heart, and more chest contents (lungs) are between the heart and the electrode.
Once your students understand what the ECG "should" look like, it is time to teach the abnormalities. Poor R wave progression (a not-very-helpful term) can be caused by a number of things, such as electrode misplacement, anterior M.I. with pathological Q waves, and chamber enlargement. For an excellent discussion of poor R wave progression, visit Life In the Fast Lane.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
A Normal ECG- Pearls on R Wave Progression/Lead Placement
Ken Grauer, MD www.kg-ekgpress.com [email protected]