
Submitted by Dawn on Thu, 03/19/2015 - 14:42
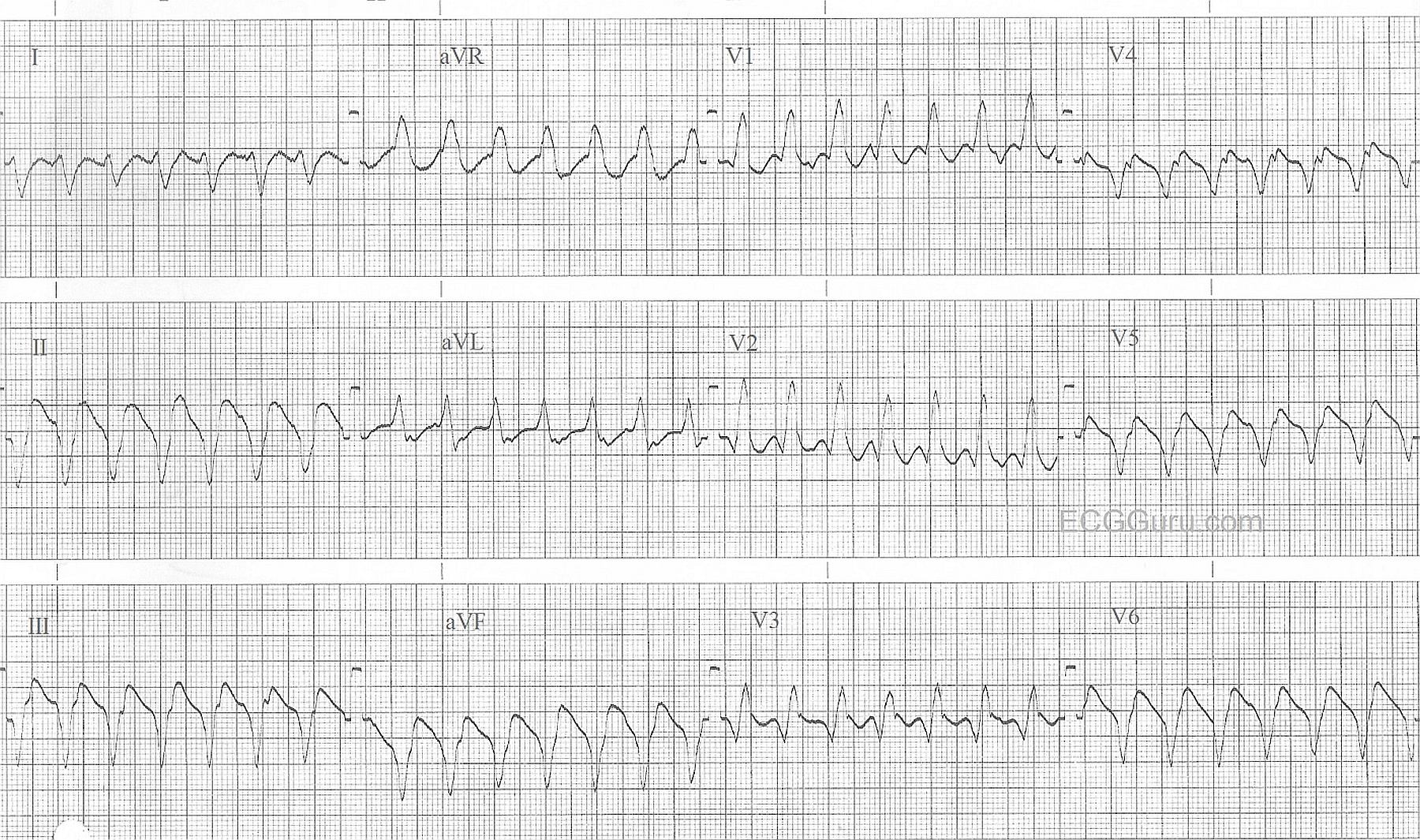
This wide-complex tachycardia is ventricular tachycardia. Along with the wide QRS and the fast rate, features which favor a diagnosis of VT over BBB include: backwards (extreme right) QRS axis, negative QRS in V6, and an apparently monophasic QRS in V1, as opposed to the rSR' pattern of right bundle branch block.
Remember, ALL wide-QRS tachycardias should be treated as V Tach until proven otherwise, as it is a life-threatening arrhythmia. Factors which lower cardiac output during V Tach include: Fast rate, wide QRS, and lack of P wave preceding the QRS. The sudden severe lowering of perfusion that usually accompanies V Tach can lead to rapid deterioraton and ventricular fibrillation.
For discussions by Jason Roediger (ECG GURU extroidonairre) on recognizing ventricular tachycardia, go to this LINK, and this LINK.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
99+% Likelihood of VT
I would interpret the ECG in the above Figure as follows:
For full Review of the above Criteria — Please check out my ECG Blog #42 (GO TO — http://tinyurl.com/KG-Blog-42 ).
Ken Grauer, MD www.kg-ekgpress.com [email protected]