
Submitted by Dawn on Thu, 07/16/2015 - 15:12
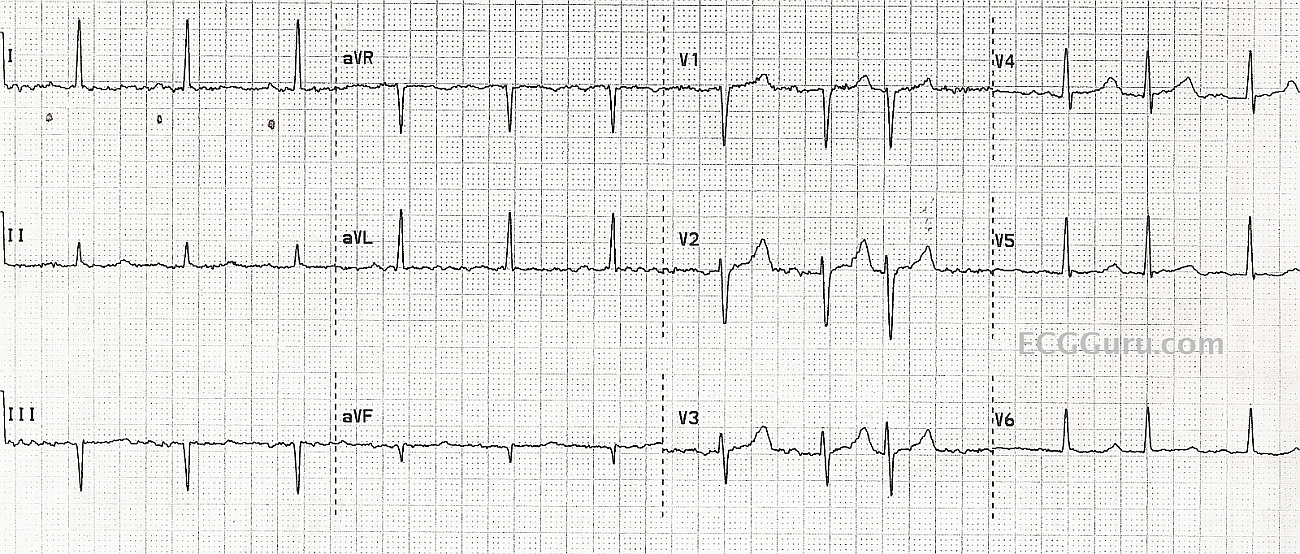
This patient was diagnosed by the rescue crew as having atrial fibrillation, based on the fact that they thought the rhythm was irregular, and they could not see P waves. They also noted a wavy baseline, and considered it to be fibrillatory waves. In reality, the underlying rhythm is regular, with some PACs (regularly irregular). The P waves are small and hard to see in the baseline artifact. We have marked the P waves in Lead I with small dots.
It pays to look at multiple leads, reduce artifact as much as possible, and look at the strip for evidence of an underlying rhythm.
It is not shown here, but the ECG machine is often able to show that the P waves are present by giving a PR interval and P wave axis in the diagnostics.
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
CHALLENGE: Is this AFib or Sinus Rhythm with PACs ???
Ken Grauer, MD www.kg-ekgpress.com [email protected]
Additional info
thanks so much, Dr. Ken. I should have added the information that the subsequent ECG in the Emergency Dept. Clearly showed sinus rhythm with occasional PACs. That tracing has been misplaced, unfortunately. I hoped to make a point that a sub-optimal ECG, with artifact, makes it nearly impossible to make an accurate interpretation.
Dawn Altman, Admin