
Submitted by Dawn on Sun, 02/24/2013 - 12:24
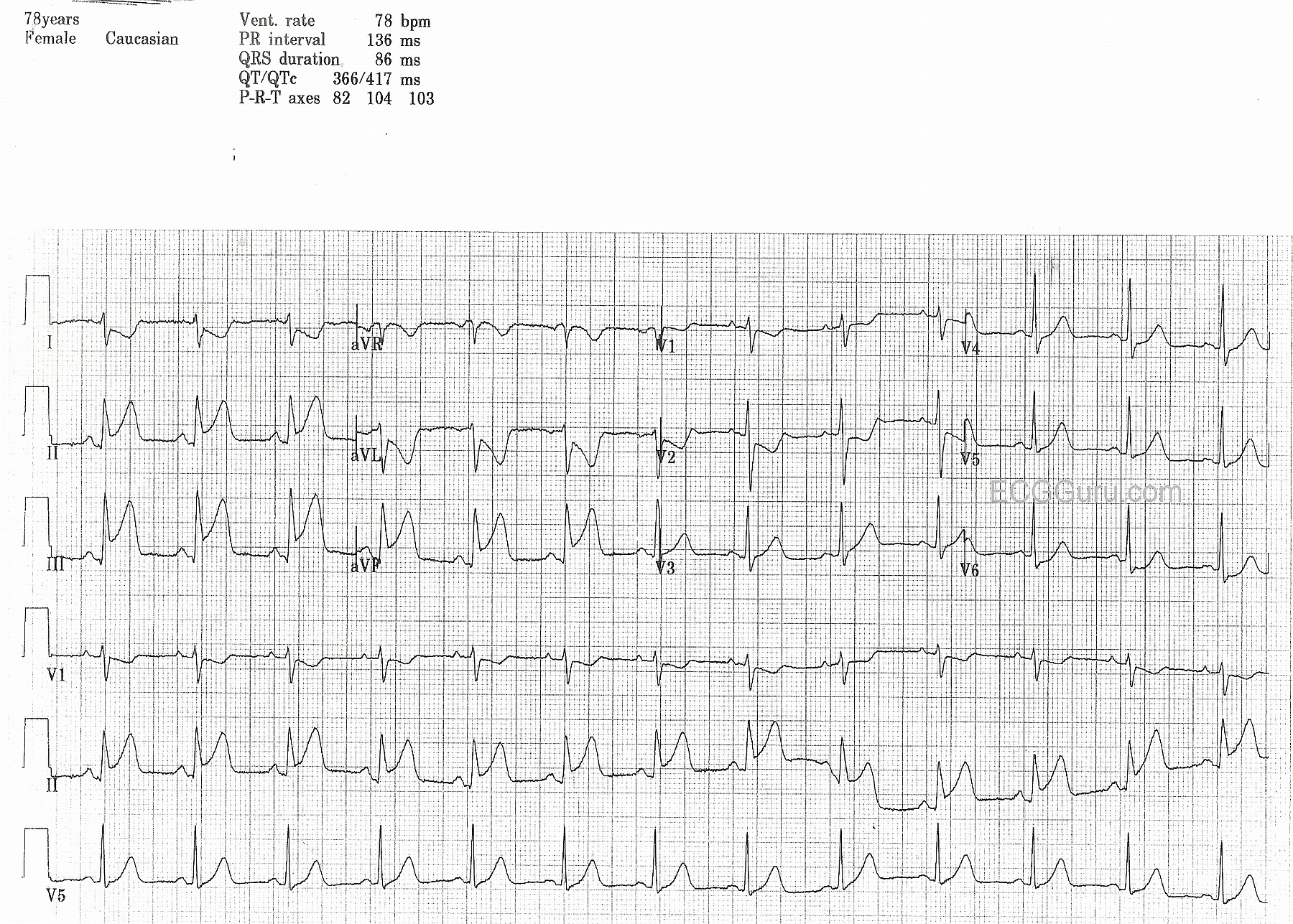
This is an excellent example of acute inferior wall ST elevation M.I. (STEMI) in a 78 year old woman who had been experiencing intermittent chest pain for two days. This 12-lead ECG has been formatted to simultaneously produce three rhythm strips below the 12-Lead. The rhythm strips are run simultaneously with the 12-Lead, and show 3 different leads. This feature can been invaluable when trying to decipher complex rhythms.
In this case, the patient is in normal sinus rhythm, and has classic ST segment elevation in the inferior wall leads: II, III, and aVF. There is some reciprocal ST depression in Leads I and aVL, and also in V1 and V2, suggesting injury extending up the posterior wall. ST depression is noticeable in V6 as well. This patient's RCA lesion was opened and stented, and she did well immediately post cath. We have no records past that.
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Acute Infero-Poster MI - with Proximal RCA Occlusion.
GREAT example of acute inferior STEMI by Dawn from a patient who interestingly had chest pain for 2 days (!) - emphasizing the point that more than just duration of symptoms may provide indication of the need for acute reperfusion. I'll just add a few points to Dawn's description.
Ken Grauer, MD www.kg-ekgpress.com [email protected]
Thank you Dawn for sharing this nice EKG and thank you Ken for adding the bright clinical light to the scene, which makes this EKG look so vivid.