
Submitted by Dawn on Sat, 02/11/2012 - 17:39
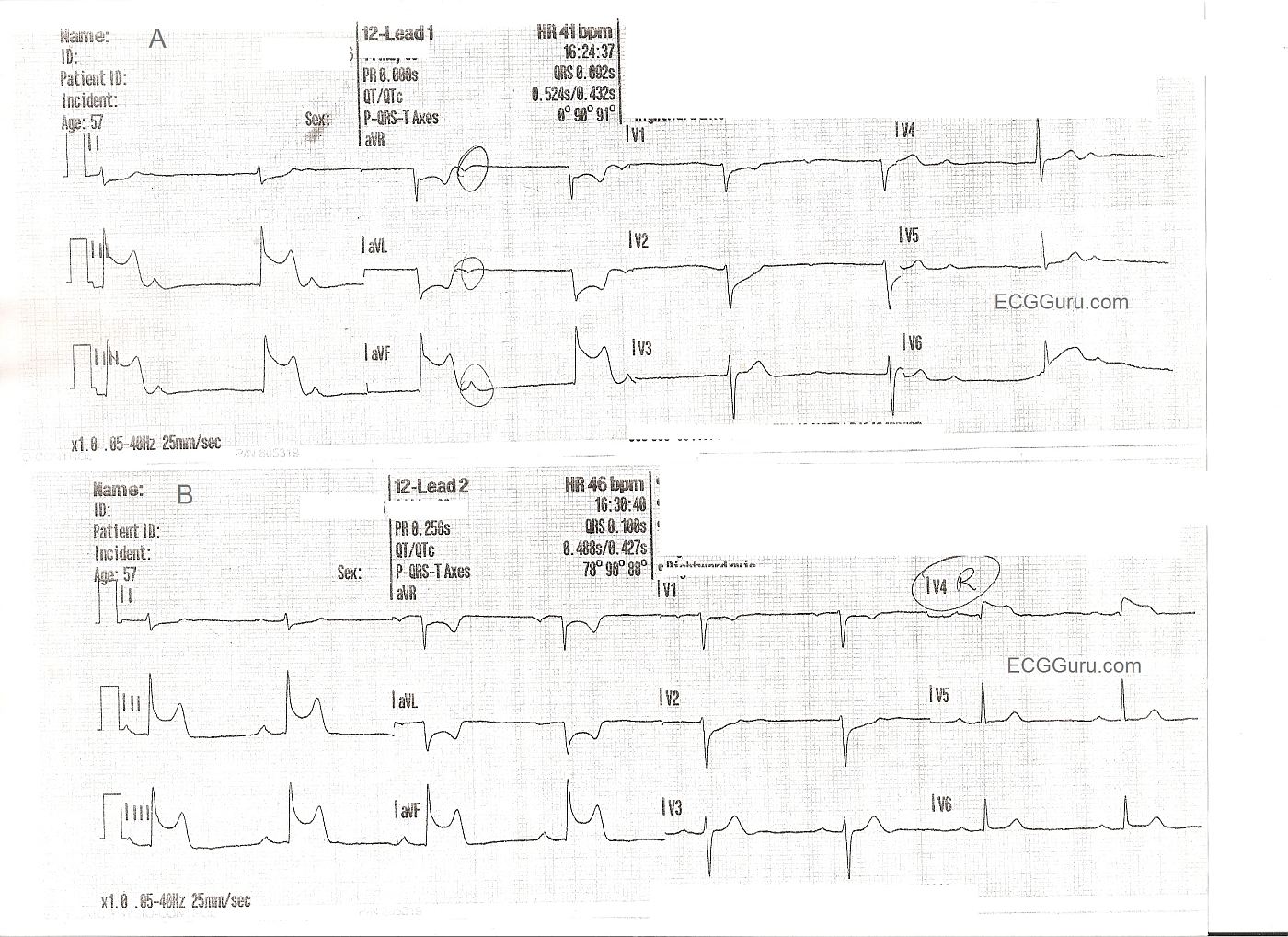
These two ECGs are from a 57 year old man with chest pain. The initial ECG shows ST elevation in Leads II, III, and aVF - inferior wall STEMI. Reciprocal changes are as expected in I and aVL. Reciprocal ST depression also seen in V1 and V2 indicate probable posterior wall involvement. Not surprising since the inferior wall is simply the lower part of the posterior wall. The first ECG also shows the patient in sinus brady with junctional escape: AV dissociation. The sinus node is often affected in IWMI that is caused by right coronary artery occlusion. The second ECG shows a slight increase in the sinus rate, and a sinus bradycardia. A V4 right lead has been performed, clearly showing ST elevation, and indicating right ventricular M.I.
FOR MORE INFORMATION ABOUT RIGHT VENTRICULAR M.I.,
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
What rhythms it cannot be
When working on the possible rhythms for the first 12-Lead, most folks should initially include a junctional rhythm with a long RP and a markedly prolonged 1st degree AVB. The former is excluded due to upright P-waves in lead II and the latter thru a changing PR interval.
In this case a trial of atropine may be indicated to speed the sinus rate while a temporary pacemaker is prepared if the patient becomes hemodynamically unstable.
Great case!
Christopher
sixlettervariable.blogspot.com
ems12lead.com
Rhythms
Thanks, Christopher. I agree with your comments. I believe the second ECG, showing a slightly faster sinus rate, establishes that the first one was sinus brady, with the junction escaping due to the slow rate. It remains to be explained why the sinus p waves did not conduct - probably in the refractory zone. I welcome more input from the ECG Gurus out there on this interesting rhythm.
Dawn Altman, Admin