
Submitted by Dawn on Sat, 11/12/2016 - 21:01
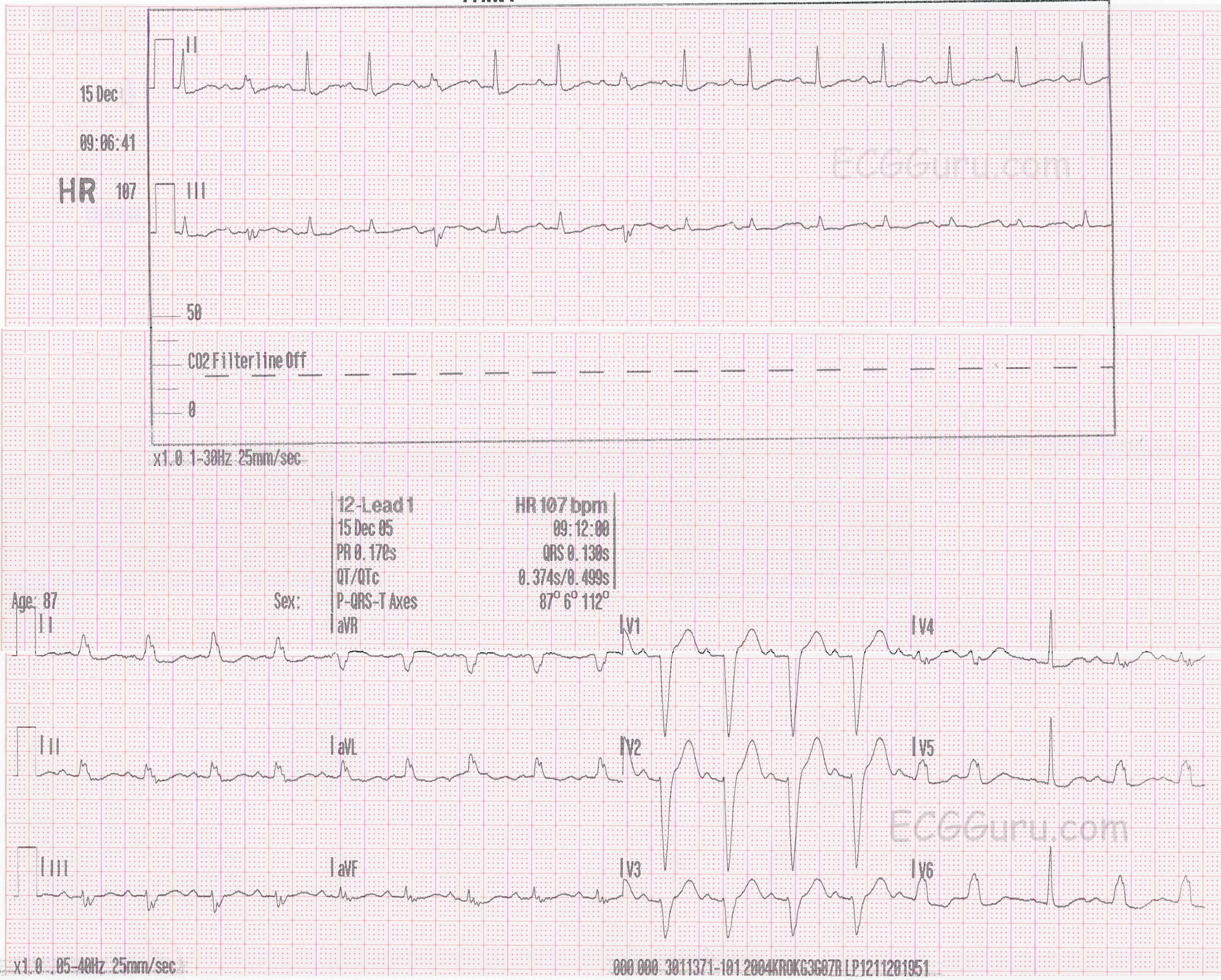
Today's ECG CHALLENGE offers a two-lead rhythm strip and a 12-lead ECG from an 87 year old man with a complaint of shortness of breath. We do not know any other clinical information. What is the underlying rhythm? How can we explain the changing QRS morphology? There are two distinctly different QRS complexes - one wide and one narrow. Comment below and let us know what you think. We will answer your questions as soon as we can, and will give a final diagnosis in one week.
ANSWER: Please see Dr. Grauer's comment below for the diagnosis. The intermittent left bundle branch block that is seen in this strip appears in the 12-lead ECG to be rate-related. That is, after a PAC, we see a pause, and then normal conduction for one beat. As the rate increases, the left bundle branch block resumes. The rhythm strip, which was recorded about 5 1/2 minutes before the 12-lead ECG, shows more intermittent normally-conducted beats, which don't seem to be rate-related. We would need a longer rhythm strip to definitively prove rate-related left bundle branch block, but it is a very common cause of intermittent LBBB.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Recognizing Rate-Related Conduction Defects
SPOILER ALERT = My Answer to this Interesting Case: The KEY lies in the last 3 leads (V4,V5,V6) of the 12-lead tracing with simultaneously-obtained 3-channel recording. Earlier in the 12-lead ECG — the rhythm is regular sinus tachycardia at 110/minute with LBBB. The 2nd beat in leads V4,V5,V6 occurs early. Because there is underlying artifact and some baseline movement — it is impossible to determine if the P wave preceding this 2nd beat in V4,V5,V6 is preceded by a different-morphology P wave (ie, a PAC) — but it is my strong hunch that this is what happens. Then the 3rd beat occurs slightly later, being preceded by the longest R-R interval on this ECG. Note that this 3rd beat in V4,V5,V6 is narrow and preceded by a P wave. Presumably, this reflects resumption of sinus rhythm after the slight pause due to the PAC that occurred just before it. Following this 3rd beat in V4,V5,V6 — the rate increases again, and LBBB conduction resumes. So presumably the reason for the wide QRS complex on this tracing is rate-related LBBB.
There are a number of interesting points to make about rate-related BBB. #1) — Clinical significance is essentially the same as for persistent BBB. #2) — Rate-related BBB is often an extremely challenging diagnosis to make — since we cannot prove this diagnosis unless we clearly see onset of a conduction defect with increase in heart rate — and resolution of that conduction defect when the rate slows back down. #3) — Diagnosis of rate-related BBB is made even more difficult by the reality that the “rate of onset is often not the same as the rate of offset”. By this I mean that rate-related BBB may develop when the sinus rate increases from 60 to 90 or 100/minute — but after the BBB develops — the rate may need to drop down to far below the 90-100/minute range before the conduction defect will resolve. As a result, it becomes challenging to “prove” that the change in rate is the responsible causative factor. For example, in the 2-lead rhythm strip we see in this case (above the 12-lead) — the rate does not appreciably change, yet we see intermittent LBBB conduction. It would be impossible to diagnose “rate-related” BBB from this short rhythm strip alone. To be certain of my hunch — I’d actually need much more monitoring than what we are given in the 12-lead tracing below it, as I’d need to see over time that rate increase reliably leads to onset of a conduction defect that eventually goes away after the rate again slows down.
Ken Grauer, MD www.kg-ekgpress.com [email protected]