
Submitted by Dawn on Tue, 08/27/2013 - 15:03
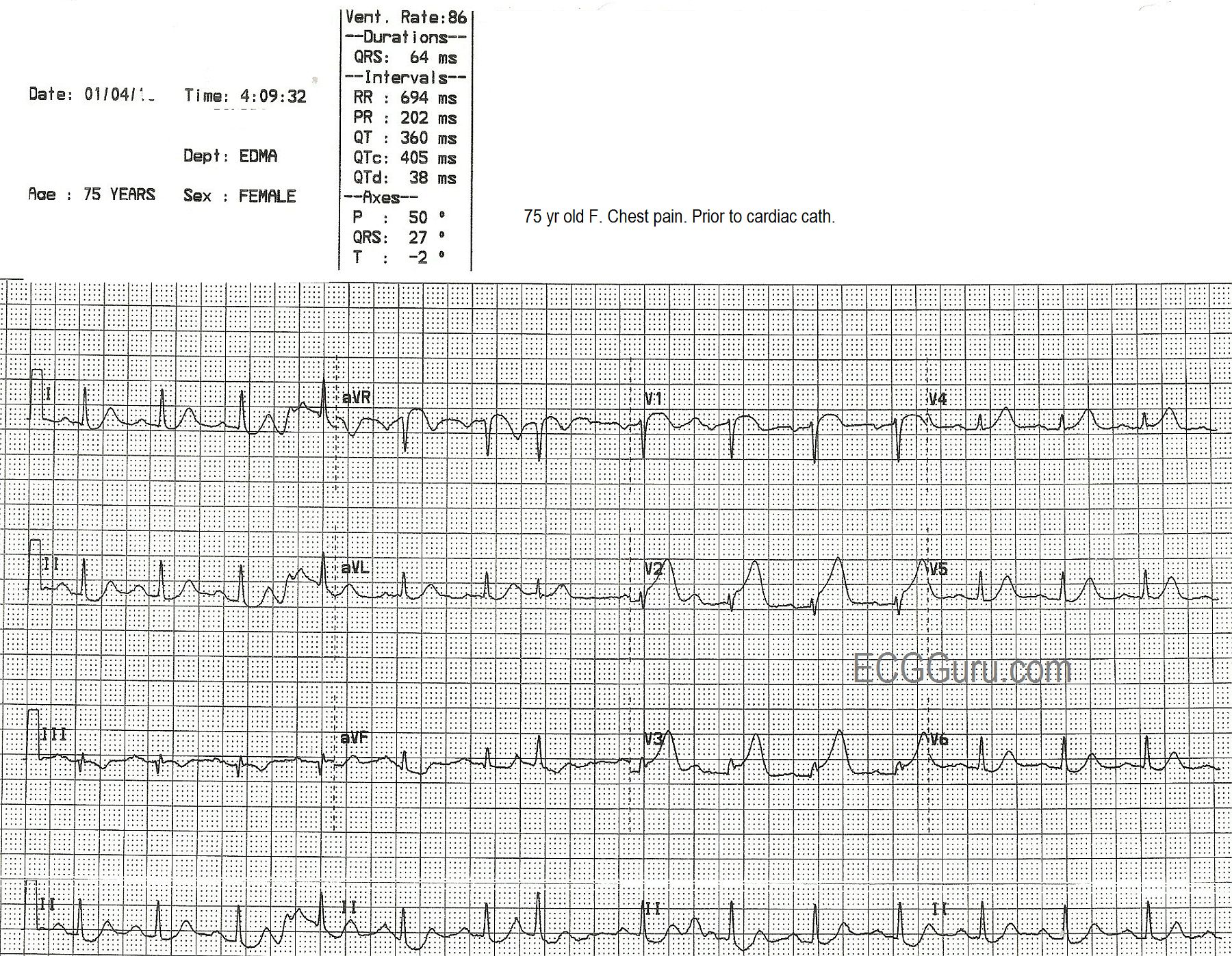
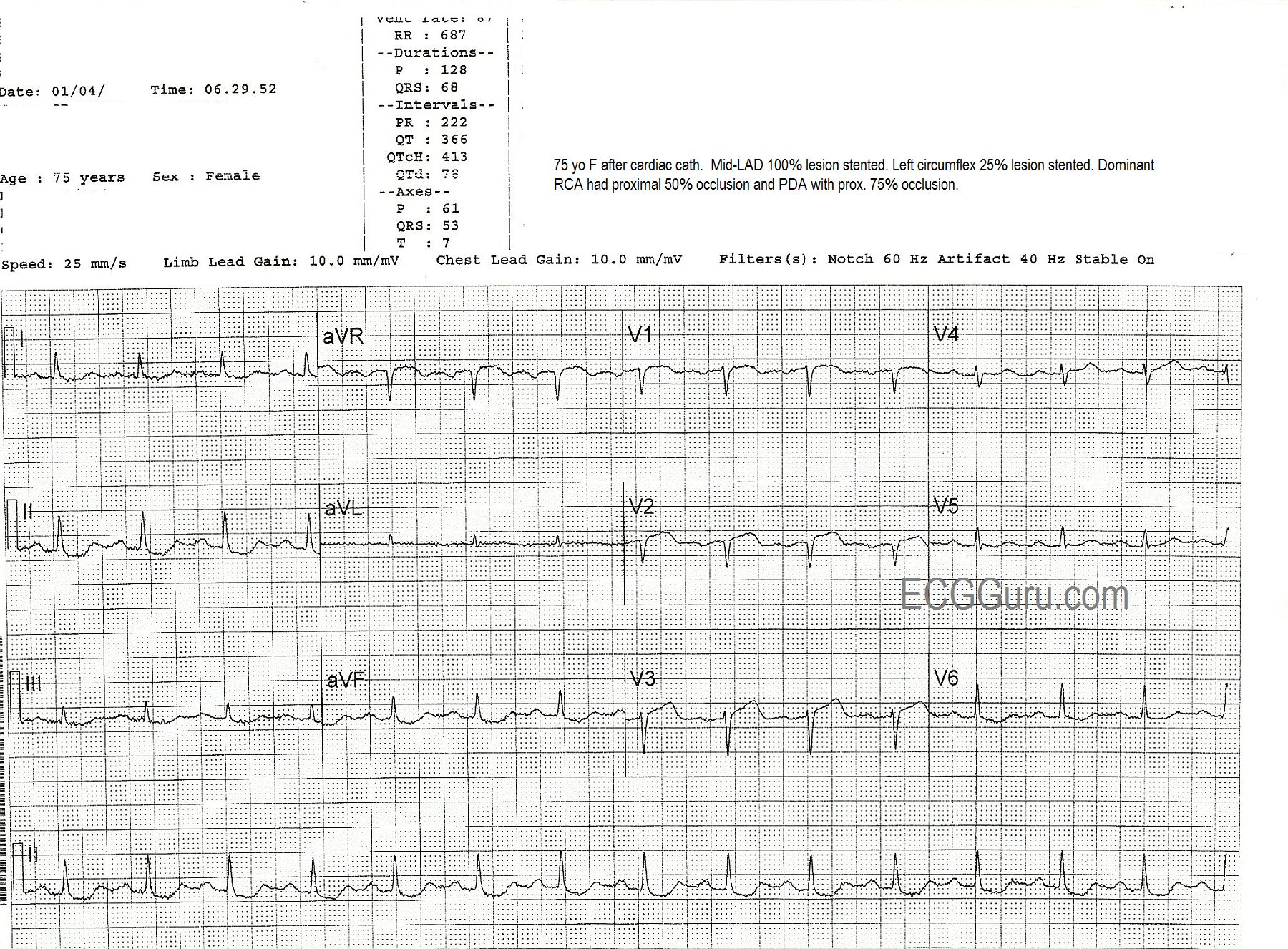
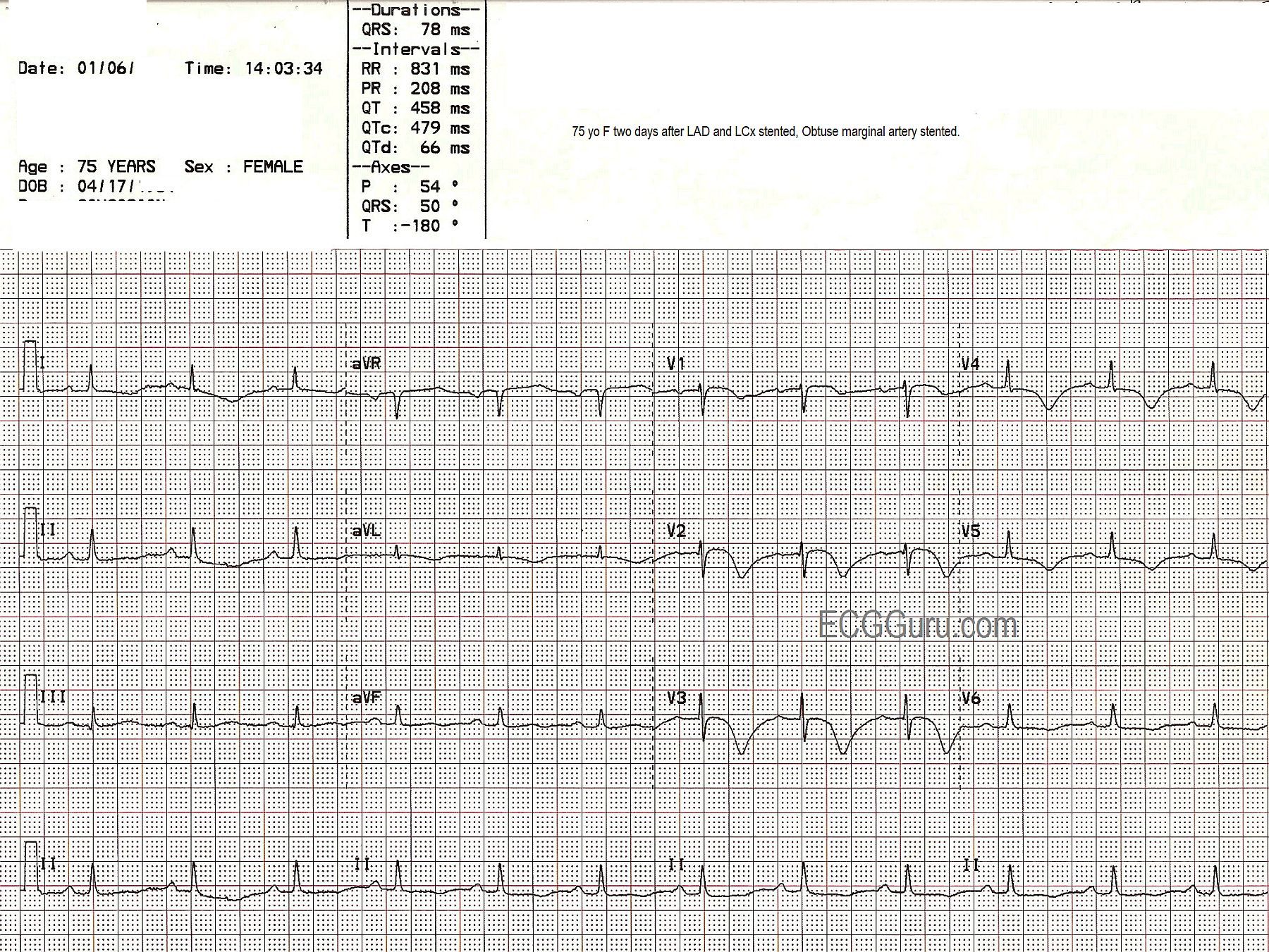
This series of three ECGs is from a 75-year-old woman who came to the Emergency Dept. with chest pain. The first ECG shows ST elevation in V1, V2, and V3, with generally low voltage in the QRS complexes. There is some coving upward of the ST segment in aVR, which can suggest a very proximal lesion of the left coronary artery (LCA). She was taken to the cath lab, where it was discovered that she had a 100% occlusion of the midportion of the anterior descending branch of the left coronary artery, which was repaired and stented. The second ECG, taken after the angioplasty, shows some Q waves in V1 and V2, with poor R wave progression in the V leads. A 25% occlusion of the obtuse marginal branch of the circumflex artery was stented two days later. The third ECG was obtained after that procedure. It shows that the Q waves have disappeared in the anterior leads (possibly due to different technicians performing the ECGs with different lead placement). It also shows marked T wave inversion in I and aVL, representing ischemia in the lateral wall, and in all the chest leads, representing ischemia in the anterior wall. The QTc is prolonged in this third ECG at 479 ms. It is not known what medications the patient was on. This patient also had a 50% proximal occlusion in the RCA and a 75% occlusion in the posterior descending artery. This is a good example of a patient with extensive coronary artery disease who finally presented for treatment when she developed ST elevation M.I.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Serial Tracings in a Patient with Acute Anterior STEMI
This case is interesting for the changes in these 3 serial ECGs. It is also interesting in that we KNOW cath findings and find ourselves almost backward trying to correlate what we see on which tracing given what was found on cath ....
Remarkable findings in ECG #1 include:
ECG #2 - was obtained after cath and stenting of the mid-LAD 100% lesion. Remarkable findings include:
ECG #3 - was obtained 2 days later after stenting of a branch of the Circumflex artery (I'm not sure we know full circumstances of this - as normally a 25% lesion as is mentioned would not be stented ... ). Remarkable frindings on ECG #3 include:
Ken Grauer, MD www.kg-ekgpress.com [email protected]
Regarding second cath...
So true, Dr. Grauer, the 25% lesion would not warrant another procedure. Alas, even though I took care of this patient in the recovery area of the cath lab, I can't remember all the details. On review of the notes I hastily wrote on the ECGs that day, the second procedure was shunting of the circ. I know her RCA had serious lesions, but I believe that was addressed at a later date. I will return to the cold, dusty vault, and see if I can find images of one or both caths.
Dawn Altman, Admin
Regarding 2nd Cath
NOT a problem Dawn! I have too-numerous-to-count tracings "in the file" that years after are lacking in details of their occurrence. I just wanted to make the point that other circumstances (beyond a 25% lesion) must have been present to prompt the 2nd procedure. That said - this is a GREAT case, and so nice to be treated to serial tracings and definitive cath results. THANK YOU!
Ken Grauer, MD www.kg-ekgpress.com [email protected]