
Submitted by jer5150 on Sat, 03/02/2013 - 09:51
Patient's clinical data:
73-year-old white man.
Rate this content:
-

- jer5150's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Unusual
I'm struggling to explain this one. There is an underlying sinus rhythm with LBBB, but there are premature beats with normal conduction. The premature beats are preceded by P waves which are different in shape from the sinus rhythm P waves and associated with a shorter PR interval, so I assume they are of atrial origin, but why is the associated QRS narrow? Could it be because of supernormal conduction in the left bundle branch? Is such a thing even possible? Following the atrial premature beat, the next sinus P wave is delayed slightly, as is usually the case, and the QRS is again of normal width. This is easy to explain by assuming that the LBBB is rate-dependent and that, given enough time, such as is provided by a post-ectopic pause, the LBB is capable of conducting.
So my initial guess is sinus rhythm with rate-dependent LBBB and atrial premature beats with supernormal LBB conduction. However, I may yet change my mind!
Dave R
Jason Fascinoma - Rate-related LBBB, Supernormal Conduction
Two things I can usually count on from this excellent ECG Weekly Challenge:
I was about to post my interpretation of this when I saw Dave's first. I agree completely:
I'd LOVE to see this patient's ECG when the PACs stop. It may well show "persistent" LBBB at such time (if the baseline sinus rate is at all a bit fast) — when in fact the patient really has rate-related LBBB.
NOTE: A Key point about rate-related BBB is that rate of onset is not necessarily the same as rate of offset. That is — you may develop rate-related BBB at a rate of 80 or 90/minute — but may need to drop back down to a rate under 70 in order for it to disappear. As might be imagined — this makes diagnosis of rate-related BBB that much more challenging! GREAT case !!!
Ken Grauer, MD www.kg-ekgpress.com [email protected]
Super Duper Conduction
Again, beautiful EKG. Seriously Jason, do you have EKG's with ALL the possible EKG findings in a folder?
I didn't see many EKG's showing this anomaly (like Dave and Ken, I too believe we're looking at a possible super normal conduction case), so I got excited when I saw it, but then I read the comments and I saw everything nicely explained already...
I might add that the LBBB (likely rate related) is somewhat expected as the patient has a constant LAFB (looks like all beats have it regardless of their rate/prematurity). So basically this is just an intermittent LPFB (probably rate related), but because of the underlying LAFB, the QRS length/morphology changes so evidently (it becomes a full blown LBBB). There's also LAE noted on this EKG, but the highlight is obviously the "super normal conduction" in the posterior fascicle seen on beats 2,6 and 10. BTW, is there an explanation of the physiology behind this interesting phenomenon?
P.S. Gotta love Ken's subject line
Not Quite LAHB ...
@Cristian - Glad you like my subject line! - : )
Realizing that there are MANY opinions as to what constitutes LAFB (alternatively known as LAHB) - to me, the beats without LBBB in this tracing do not qualify ... Mean QRS axis should be at least -30 degrees by any criterion that is used to qualify for LAHB — and the R > S in lead II of Jason's tracing (ergo, mean axis is negative but less negative than -30 degrees).
I hope the above is helpful.
Ken Grauer, MD www.kg-ekgpress.com [email protected]
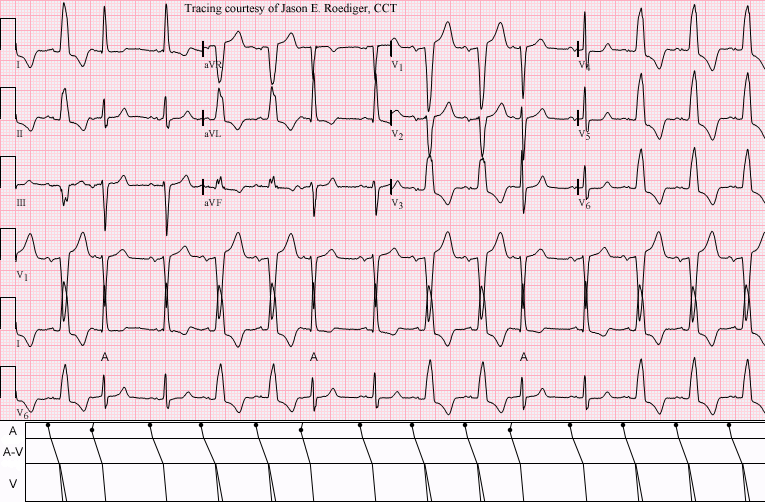
INTERPRETATION
INTERPRETATION:1. Sinus rhythm (rate about 86/min) interrupted by frequent . . .
2. . . . atrial premature beats (APBs; 7th, 6th, and 10th beats) with . . .
3. . . . supernormal conduction through the left bundle branch (LBB).
4. Critical rate-dependent left bundle-branch block (LBBB).
5. Left ventricular hypertrophy (LVH).
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]
intermittent LBBB with PACs
Thanks for a interesting ECG.
I suppose following: Basic rithm is sinus rhythm with intermittent LBBB (1st, 4th, 5th, 8th, 9th, 12th, 13th, 14th-sinus beat with LBBB). 2nd, 6th, 10th beats are premature atrial contracion.
Mari
My ECG , exact moment of RBBB->LBBB captured on ECG
HI there
Have a look at this:
dl.dropboxusercontent.com/u/32778364/exact-moment--change-to-LBBB.jpg
Always had a RBBB. Since last week, presented with LBBB, CK non-elevated, echo normal. persists.
Managed to get one good without LBBB. next day again LBBB.
What you see is the exact moment of transition. If I was holding breath, no LBBB. Only when I started breathing.
Any clues?
thanks in advance. I am film editor, so not very much into this, but learning :)
Igor
Rate-Related LBBB
Hello Igor. The purpose of the ECG Guru is to provide a medium to foster education in ECG interpretation. It is not aimed at giving medical advice. I suspect your tracing shows a rate-related LBBB - though resolution/slight curvature of the paper make it difficult to be sure. I strongly suggest you see your personal physician regarding you ECG changes. Your physician may or may not refer you to a cardiologist. Wishing you the best.
Ken Grauer, MD www.kg-ekgpress.com [email protected]