
Submitted by jer5150 on Sat, 06/09/2012 - 17:38
From June 10, 2012: As is the case with all practical blogs, I’m encouraging ECG Guru members to engage in active group participation. Share your thoughts, observations, impressions, findings, and interpretations. Feel free to compare notes with one another and pick each other’s brains.
Please post your comments and inquiries and I guarantee I'll respond to them in a timely manner as soon as they are received (usually within a few short hours). All questions will be answered and the interpretation (accompanied by laddergram) will be revealed on Sunday, June 17 2012 at which time I will post a brand new Case of the Week.
Rate this content:
-

- jer5150's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
I believe this is a SNRT (P
I believe this is a SNRT (P morphology almost identical to that of SR) that abruptly stops thanks to a APC (you can see it in the T wave of the last beat of the tachycardia).
APCs! You're on the right track and getting warmer.
The first half of the ECG has a rate that is marginal at exactly 100/min, so the first 8 beats represent a regular Normal Sinus Rhythm. The rate is borderline, yet not fast enough to qualify as a true tachycardia. Sinoatrial Nodal Reentrant Tachycardia (SNRT) is certainly on the short list as a differential diagnosis to be considered. There’s a mechanism known as Inappropriate Sinus Tachycardia (IST) that might also be considered as a differential.
You’ve made a couple of keen observations regarding the morphology of the sinus P-waves preceding each QRS complex. They’re all identical and each of the 13 fully-conducted beats is originating in the sinus node.
Good pickup on the Atrial Premature Complex (APC). Does the APC have a more specific name? In other words, is the APC: 1.) normally conducted, 2.) aberrantly conducted, or 3.) nonconducted?
Is there only one (i.e., singular APC) or are there others (i.e., plural APCs)?
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]
Is this Tachy-Brady Syndrome?
Looks like sinus tachycardia (100bpm) with sudden change to sinus brady. In presence of RBBB (RSR in v1) and Left anterior hemiblock (LAD). No other explanation for LAD (ie no evidence of LVH, inf MI, ?COPD) so could result from recent anteroseptal MI? Check History?
HCW
"Cherchez le P"
Tachy-brady syndrome is a good guess but this isn’t due to any manifestation of sick sinus syndrome or sinus node dysfunction.
What looks like sinus bradycardia is actually something that is “mimicking” sinus brady. There are only a couple of things that can simulate sinus brady to near-perfection. The late Dr. Marriott used to call these “Mutual Mimics”. Whenever you see what you believe is sinus bradycardia, you should think of its mimic and exclude it as a possibility. There is a left axis deviation (LAD) due to the LAHB. The bifascicular block is unrelated and not directly contributing to the change in the rate.
Hint: The sinoatrial (S-A) node is not speeding up or slowing down nor is it changing its own rate in any way. Something extrinsic to the S-A node is interrupting its regular discharge and causing it to reset. You might have to strain your eyes, but the answer here lies in a very subtle waveform. In French: “Cherchez le P”.
Sometimes the only way to obtain an definitive answer is by the process of elimination. If you can systematically exclude all other possibilities, then the last thing that remains on the list must be the answer. Now that we have excluded SNRT and tachy-brady syndrome as the answer, there are only about 3 other causes remaining and it is one of those 3 that is the answer here. There are many "mimics" in electrocardiography and this is one of the most convincing.
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]
There is notch on T wave of
There is notch on T wave of 8th complex I think this is PAC ,and that's not conducted .then normal pqrs like 2 and dgree avb for 5 cycle runs
Imad
Now put all of the clues together.
Your initial observation is absolutely correct Imad. The notch that is deforming the ST-segment of the 8th beat is an ectopic atrial impulse that is not conducted to the ventricles. The best descriptive term for such a beat is to call it a nonconducted PAC (or nonconducted APB). The most common cause of a sudden, unexpected pause is always going to be a nonconducted PAC. Statistically they are much more common than any of the other mechanisms that create or generate pauses such as sinus pause, sinus block, or sinus arrest. Whenever you see a pause or break in an otherwise regular rhythm, the very first thing that you should think of is a nonconducted PAC. Even other causes of pauses such as Type I and Type II A-V blocks are not nearly as common as nonconducted PACs. If just one nonconducted PAC was able to generate a pause (i.e., longer RR interval) between the 8th and 9th beats . . . . what would happen if that pattern of pauses continued to subsequently repeat itself after every sinus beat? What name would we give to such a repeating pattern and call that rhythm mechanism? This is not due to any form, type, or manifestation of block (whether it be S-A or A-V). I'm still trying to refrain from giving away the complete answer just yet. However, as Guru members spot individual details, I do want to reinforce the ones that are right while correcting the ones that aren't.
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]
Nonconducted PAC induced
Nonconducted PAC induced inhibition of sinus node to generate new pulse,and did not throw AVN because it was in refractory period,that is cause of pause ,(nonconducted atrial bigeminy)as your mention sir
Imad
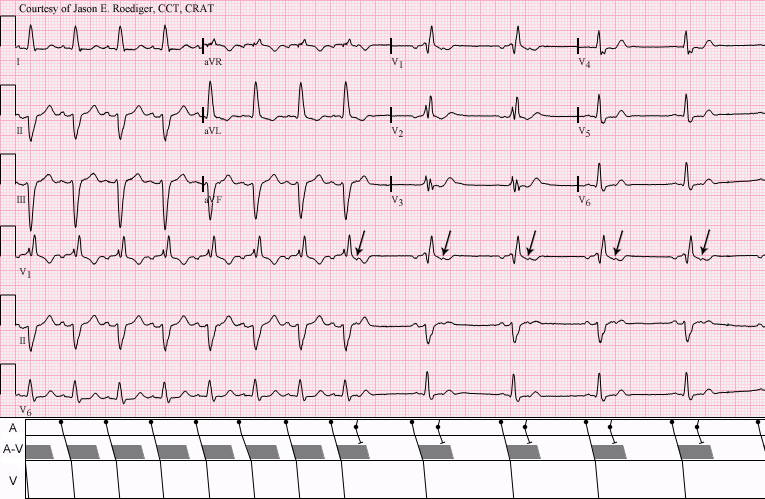
INTERPRETATION
INTERPRETATION:
1.) In first half of strip: Normal sinus rhythm (rate = 100/min) with . . .
2.) . . . bifascicular block—right bundle-branch block plus left anterior hemiblock
(RBBB + LAHB), left axis deviation (LAD) at -57 degrees.
3) In second half of strip: Sinus rhythm interrupted by a run of nonconducted atrial bigeminy
(arrows (↓); see laddergram).
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]