
Submitted by jer5150 on Sat, 02/16/2013 - 14:29
Patient's clinical data: 81-year-old black man
The computer interpreted this ECG as:
Sinus bradycardia 1st degree AV block
ST abnormality, possible digitalis effect
Abnormal ECG
When compared with ECG of (expunged)
PR interval has increased
Vent rate has decreased by 23 BPM
DO YOU AGREE WITH THE COMPUTER?
Rate this content:
-

- jer5150's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Not as simple as it first appears
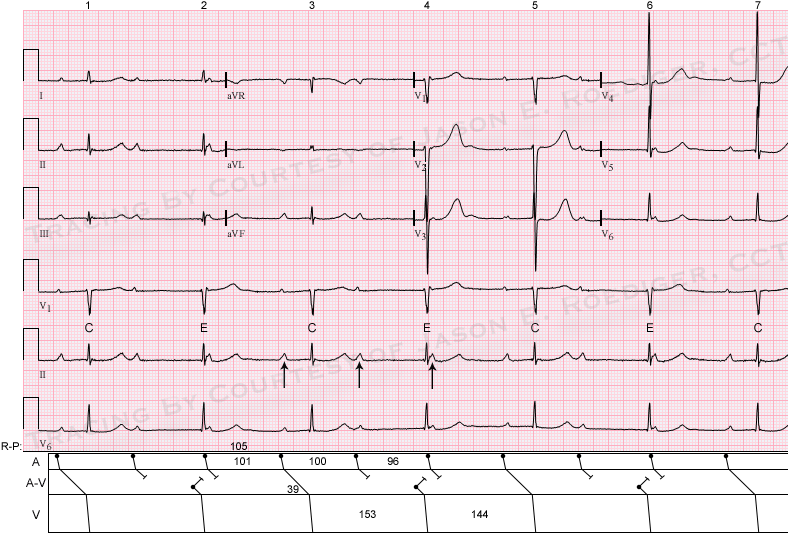
The computer is undoubtedly wrong! I'm not sure of the correct name for this rhythm but I think I know what's going on. It may look at first glance like complete heart block but it isn't. The first QRS is probably conducted with a PR interval of about 0.36s. The P wave following it is blocked and the next QRS is a junctional escape. The next P wave, occurring immediately after the QRS, cannot possibly conduct, but the next one does, again with a PR of 0.36s. The 5th P wave occurs some way after after the previous QRS, so could be expected to conduct but does not, so this one should be considered blocked. The QRS that follows is another junctional escape beat. Again there is a P wave immediately after the QRS which obviously cannot conduct; the next P wave does conduct and results in the 5th QRS. And so it goes on. The result is that capture beats alternate with escape beats in what could perhaps be described as sinus rhythm with high grade AV block and RP-dependent conduction, producing an escape-capture bigeminy. Although I think this would often be interpreted as complete heart block; the giveaway that it is not is the alternating long and short RR intervals. The escape interval is always 1.52s; the RR interval ending in the capture beat is always shorter. The other clue is that the QRS ending the shorter RR interval is always preceded by a constant PR interval (0.36s), indicating that it is a conducted beat. Jason's ladder diagram, when it appears, will make all this much easier to understand than my wordy explantion.
Dave R
2nd Degree AVB
Beautiful EKG again. Except for the rhythm disturbance, a slightly prolonged QTc and a possible RAE, no obvious abnormality jumps at me.
Now the rhythm...
Like Dave mentioned, some beats seem to be conducted 1,3,5,7 (the chances of these 4 beats having equal PRi's would be really low if they were not conducted, plus the PRi is long enough to make the P waves very good candidates for conduction), so we're not looking at a complete heart block.
Atrial rate is around 60 bpm. The slight PPi changes (the PPi's that contain the conducted QRS's are slightly longer) are probably due to an atypical ventriculophasic arrhythmia. The JEB's (beats 2,4,6) come too late to make an impression on the PPi's the contain it.
So the rhythm could be interpreted as a Second Degree AVB (can't tell which type, since we don't have 2 consecutive conducted P waves) with Junctional Escape Beats.
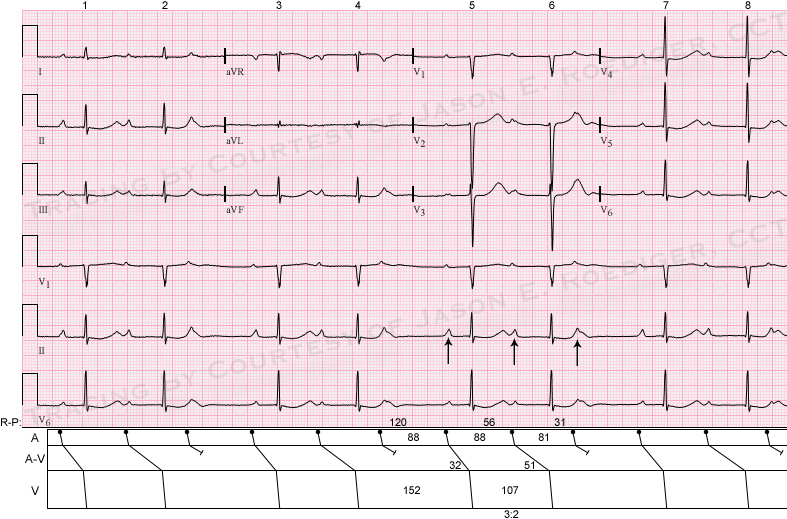
Alternately, it could be simply seen as a 3:2 Wenckebach periodicity. Although the PRi is almost a second long, it could theoretically conduct, plus it seems to be the same for beats 2,4,6.
The computer might have had a bad day... they're usually very close to the correct diagnosis.
Change of mind
After reading Cristian's comments, I now think it's his second option - simply sinus rhythm with 3:2 Wenckebach AV block.
Dave R
I'm sorry Dave, but I regret
I'm sorry Dave, but I regret to inform you that you're not allowed to reverse your position. You already called this "escape-capture bigeminy" and now you'll just have to live with your original interpretation. It's one of the unwritten rules on the ECG Guru website - so I'm going to invoke my privilege of no "take backs".
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]
Aaagh!
Aaagh!
Dave R
INTERPRETATION
INTERPRETATION (Top ECG):
1. Sinus rhythm (rate about 60/min) with . . .
2. . . . Type I A-V block manifest as . . .
3. . . . “escape-capture bigeminy” (see laddergram).
4. Ventriculophasic sinus arrhythmia.
INTERPRETATION (Bottom ECG):
1. Sinus rhythm (rate about 70/min) with . . .
2. . . . Type I A-V block manifest as . . .
3. . . . 3:2 Wenckebach periods (see laddergram).
4. Ventriculophasic sinus arrhythmia.
Here's a couple of nice examples of
escape-capture bigeminy 1.
escape-capture bigeminy 2
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]
Two bigeminies
The first ECG is a typical escape-capture one - a Wenckebach "over the top" is most unlikely at this rate. The one below is a common or garden Wenckebach. The ventriculophasic effects are irrelevant here as they should not affect the diagnosis.