
Submitted by jer5150 on Sat, 08/11/2012 - 08:21
Patient’s clinical data: 54-year-old black man. PMH significant for atherosclerotic disease, HTN, CVA, PVD, ETOH abuse, and substance abuse. Previous cardiac cath showed angiographically insignificant CAD.
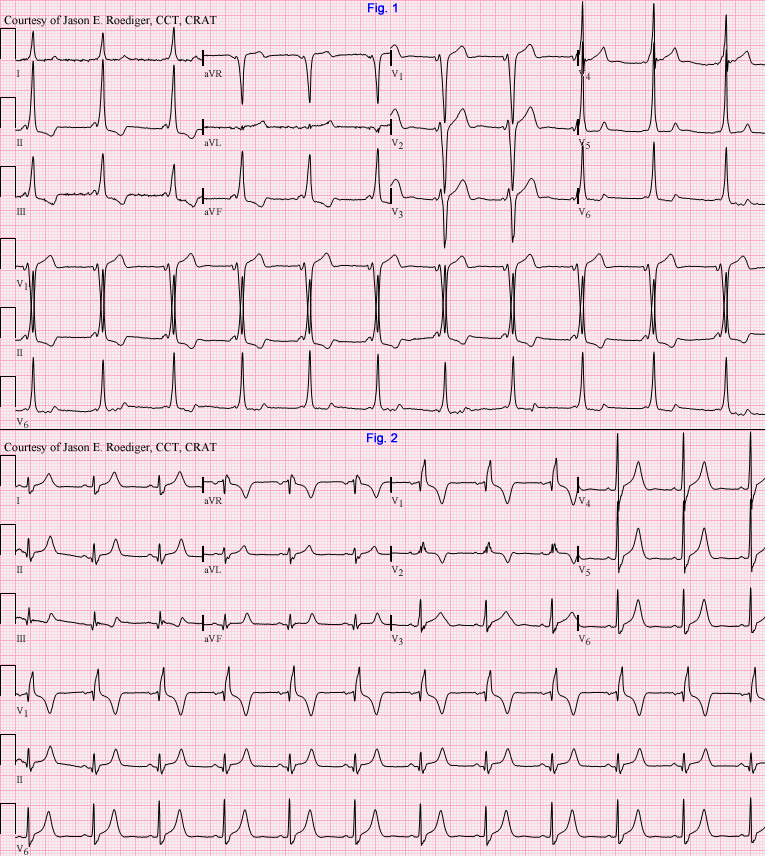
Both of these ECGs were performed just a single day apart from one another. During that intervening period of time, this patient underwent a cardiac electrophysiology (EP) study and radio frequency ablation (RFA). During the procedure, atrial fibrillation was easily induced. The pattern seen in Fig. 2 may have manifest as a direct result of the procedure or it may have been masked all along by the pattern seen in Fig. 1.
*NOTE: Prior to the procedure, all previous ECGs were consistent with Fig. 1. All subsequent ECGs were consistent with Fig. 2.
As part of its interpretations, the computer made the following statements regarding each ECG.
Fig. 1: Inferior myocardial infarction, Age indeterminate
Fig. 2: Possible inferior myocardial infarction
DO YOU AGREE WITH THE COMPUTER?
Questions:
(1.) Should we be concerned by the alteration of the QRS morphology?
(2.) Why would you not want the ECG in Fig. 1 to be combined with atrial fibrillation?
(3.) Does this patient require implantation of a permanent pacemaker?
(4.) In what way does the word "right" factor into the interpretations of both ECGs?
Rate this content:
-

- jer5150's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
The first ECG looks like a
The first ECG looks like a right anteroseptal, possibly right free wall AP. The P wave is abbreviated by the early ventricular activation and there is a LBBB pattern in the precordial leads. After ablation the patient has a right bundle branch block - probably underlying, but RBBB is common during an EP procedure due to catheter manipulation and can sometimes take days to weeks to recover. Nothing to worry about here - no indication for the pacemaker etc. Finally, there is a statistically small risk of VF in the context of preexcited atrial fibrillation.
WPW and iatrogenic RBBB
I agree with CABGPATCH.
Lown-Ganong-Levine Syndrome Vs WPW
Short PR most likely WPW can lead into AFIB and rapid decline of pt. Given age poss. ICD.
INTERPRETATION
Interpretation: (Fig. 1)
(1.) Sinus rhythm (rate = 65/min) with . . .
(2.) . . . ventricular preexcitation; Wolff-Parkinson-White (W-P-W) syndrome
Interpretation: (Fig. 2)
(1.) Sinus rhythm (rate = 68/min) with . . .
(2.) . . . right bundle-branch block (RBBB).
This patient did have W-P-W syndrome. I can only imagine that the EP docs elected to perform an invasive radio frequency ablation (RFA) because the patient was experiencing symptoms from preexcited atrial fibrillation with markedly rapid ventricular response. During the ablation, the EP doc noted the presence of a right anteroseptal accessory pathway (AP). Historically, the prodominantly negative QRS polarity in lead V1 used to be called "pattern type B". In these modern times, most EP docs don't use the designation "pattern type A" or "pattern type B" anymore although manufacturers of ECG machines continue to program those statements into the computer's interpretation algorithm. Instead, EP docs usually prefer to mention the anatomic location of the AP (e.g., anteroseptal). At the time the ablation was performed, "the pre-excitation pattern disappeared and was replaced by the baseline RBBB". In their progress note, the electrophysiologist also stated "RBBB likely catheter-induced versus baseline".
On at least one of this patient's 3 preexcited ECGs, the computer misinterpreted the QRS morphology as sinus rhythm with short P-R interval and LBBB. Patient never received a pacemaker and continued to display RBBB on their ECGs for the next 6 years. Since the RBBB never resolved, it was probably present before the ablation and was therefore permanent/fixed. It was never reported that the patient had a myocardial infarction even though the computer suggested that before and after the ablation was performed.
I got the idea for posting this case when I fortuitously came across this article during one of my random searches on Google for interesting case studies. http://www.ipej.org/1203/daisuke.pdf
If I'm not mistaken, the Post-Ablation ECG in the article has some switched precordial cables. V1, V5, and V6 are all correct but I think that V2 is really V4 - - - V3 is really V2 - - - and V4 is really V3.
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]