
Submitted by jer5150 on Sun, 02/02/2014 - 10:12
Patient data: 66-year old man.
Rate this content:
-

- jer5150's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
high grade AV block
I think this is sinus rhythm with high grade AV block and a ventricular escape rhythm, with RP-dependent conduction. Beats 3 and 6 are capture beats – the P waves here manage to conduct because they fall far enough after the previous QRS that the conduction system has had time to recover. Although beat 4 is an escape beat, there is little doubt that the P wave before it would have managed to conduct and produce a capture beat if the escape beat hadn’t intervened before the atrial impulse managed to reach the ventricles. This illustrates an important principle in high grade AV block: whether or not an atrial impulse manages to conduct depends not only on the state of refractoriness of the conduction system, ie where the P wave falls, but also on the AV conduction time and the escape interval. AV block can be a complex phenomenon.
Dave R
- Sinus rhythm @ about 65
- Sinus rhythm @ about 65 bpm with minor variation
- Indeterminate AV block that I think we can confidently call type II (two beats with different RP's conduct with equal PR's plus other clues)
- Infra-Hisian escape rhythm @ about 36 bpm.
- AV-dissociation
- Critical RP is > 930ms but < 1000ms
- First-degree AV block
- RBBB with an atypical appearance, LAFB, yielding bifasciular block
- Non-specific T-wave abnormality in the precordials in the conducted beats (upright in V1, down sloping w/ down-up biphasic in V4-V6).
Reading Dr. Richley's comment now, I would argue that this cannot be called a high-grade AV block because I don't see any two consecutive impulses that are truly "blocked."
Vince D
http://www.medialapproach.com
A terminological problem?
Interesting observations from Vince, as always. It’s true that this rhythm doesn’t fit with either of the common definitions of high grade AV block: 2 consecutive blocked P waves, or more blocked than conducted P waves. However, only 2 of the 6 beats on the ECG are conducted and this rhythm disturbance doesn’t really fall neatly into any of the standard classes of AV block. I have long thought that the standard classification of AV block is often inadequate to describe what is happening, but that’s a discussion for another day!
Vince makes the point that there is RBBB, but is there? I would argue that there is a non-specific intraventricular conduction abnormality because although there is an rsR’in V1, the 2nd R-wave is not broad; in fact if any single component of the QRS in V1 is slightly broad, it is the s-wave, and this is not typical of RBBB. Moreover, in neither I nor V6 is there any suggestion of a broad s- wave due to delayed RV activation.
I’m sure Vince and I agree over what is going on here but just use different terminology to describe it, and much of this discussion is probably somewhat academic! I think the important thing is that there is significant AV block due to advanced disease of the ventricular conduction system and that a pacemaker is probably indicated, but as usual Jason provides us with a fascinating ECG that brings up a number of interesting discussion points.
Dave R
Agree about the difference in
Agree about the difference in terminology, though we both "see" what is happening here. The key for the provider encountering this patient is that this arrhythmia is very likely due to fixed conduction disease (once you exclude DIE http://www.medialapproach.com/die-from-bradycardia/), and thus: 1) shouldn't be expected to respond to atropine, and 2) as you state, will probably require permanent pacing.
Interestingly, if this patient was in the ED he would almost certainly get a dose or two of atropine. While that wouldn't do a thing to help his infra-Hisian block, the increased sinus rate might help us on the sideline settle on a label for the block. In that case I suspect we would be seeing true high-grade AV block with multiple consecutive blocked P's, given the long crtitical RP-interval.
Regarding the RBBB, you are quite right that I should have called it a NSIVCD for the reasons listed. I was on the fence and think that nice S-wave in II, though it has absolutely no bearing on the RBBB, was subconsciouly making my think there was one in I. I suspect if we could see a supraventricular complex in I it wouldn't look like RBBB there either.
Vince D
http://www.medialapproach.com
Thanks
I don't usually comment on Jason's ECGs, preferring to "lurk" on the sideline and learn from the masters. But, I did want to say that I enjoyed the discussion between Dave and Vince, as I am always interested in AV blocks and all their nuances, and have witnessed many effective and non-effective treatments in the E.D. Thanks, guys!
Dawn Altman, Admin
Great ECG resource
Great ECG resource
INTERPRETATION
INTERPRETATION:
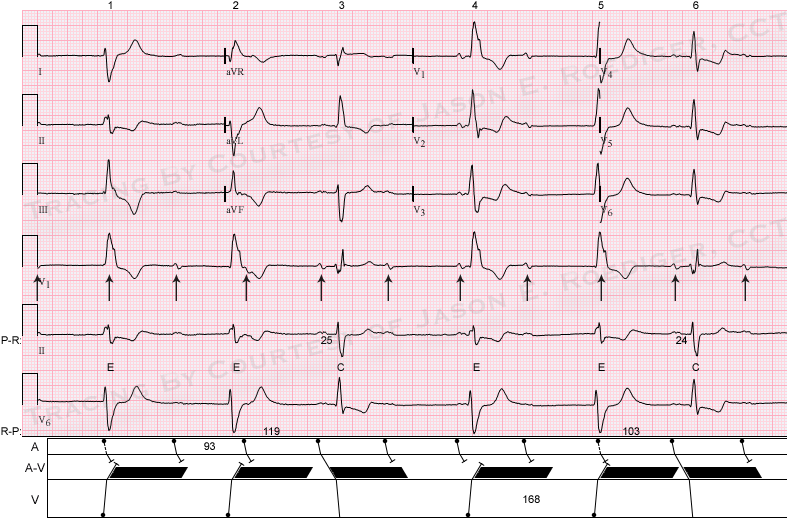
(1.) Slightly irregular sinus rhythm (rate about 63/min) with . . .
(2.) . . . some (indeterminate) form of incomplete A-V block producing . . .
(3.) . . . A-V dissociation and resulting . . .
(4.) . . . idioventricular escape rhythm (rate about 36/min) originating from the left ventricle (LV).
(5.) Two ventricular capture beats (3rd and 6th beats) conducted with prolonged P-R intervals and . . .
(6.) . . . nonspecific intraventricular conduction delay (NSIVCD).
COMMENTS:
If the sinus rate was slightly slower at a rate less than 60/min, I wouldn’t hesitate to call this a high-grade (advanced) A-V block. As is, I don’t think this technically qualifies yet as a high-grade A-V block. I agree with Vince that this is probably due to infra-Hisian block resulting in a ventricular escape mechanism distal to the site of lesion. The computer did call this a right bundle-branch block but I’m not sure if it was referring to the capture beats (C) or the escape beats (E). In either case, it’s wrong about the escape beats having a RBBB morphology. The capture beats (as Dave and Vince mentioned) would be better described as conducting with NSIVCD and not RBBB. In the laddergram, the black-shaded area represents the absolute refractory period (ARP). Conduction is only possible if the sinus impulse lands beyond this point. The 1st, 2nd, 4th, and 5th beats are ventricular escape beats that presumably originate from the left ventricle. Note the taller left rabbit ear equivalent in lead V1 with notching/slurring on the down stroke of the R-wave, rS complex in lead V6, and right axis deviation.
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]