This series of strips was donated by Arnel Carmona, and was taken from a patient admitted to the hospital for a urinary tract infection. No other history is known. On close examination of this rhythm what do we see?
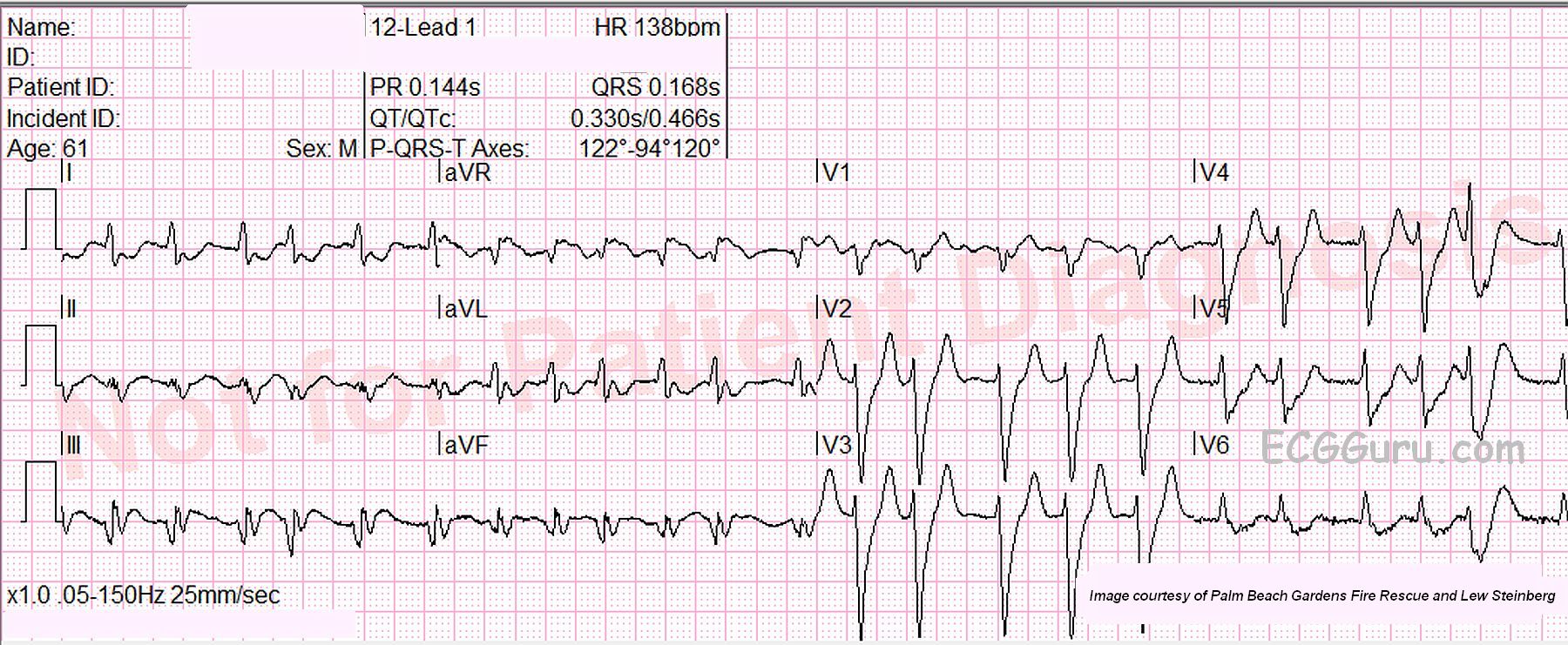
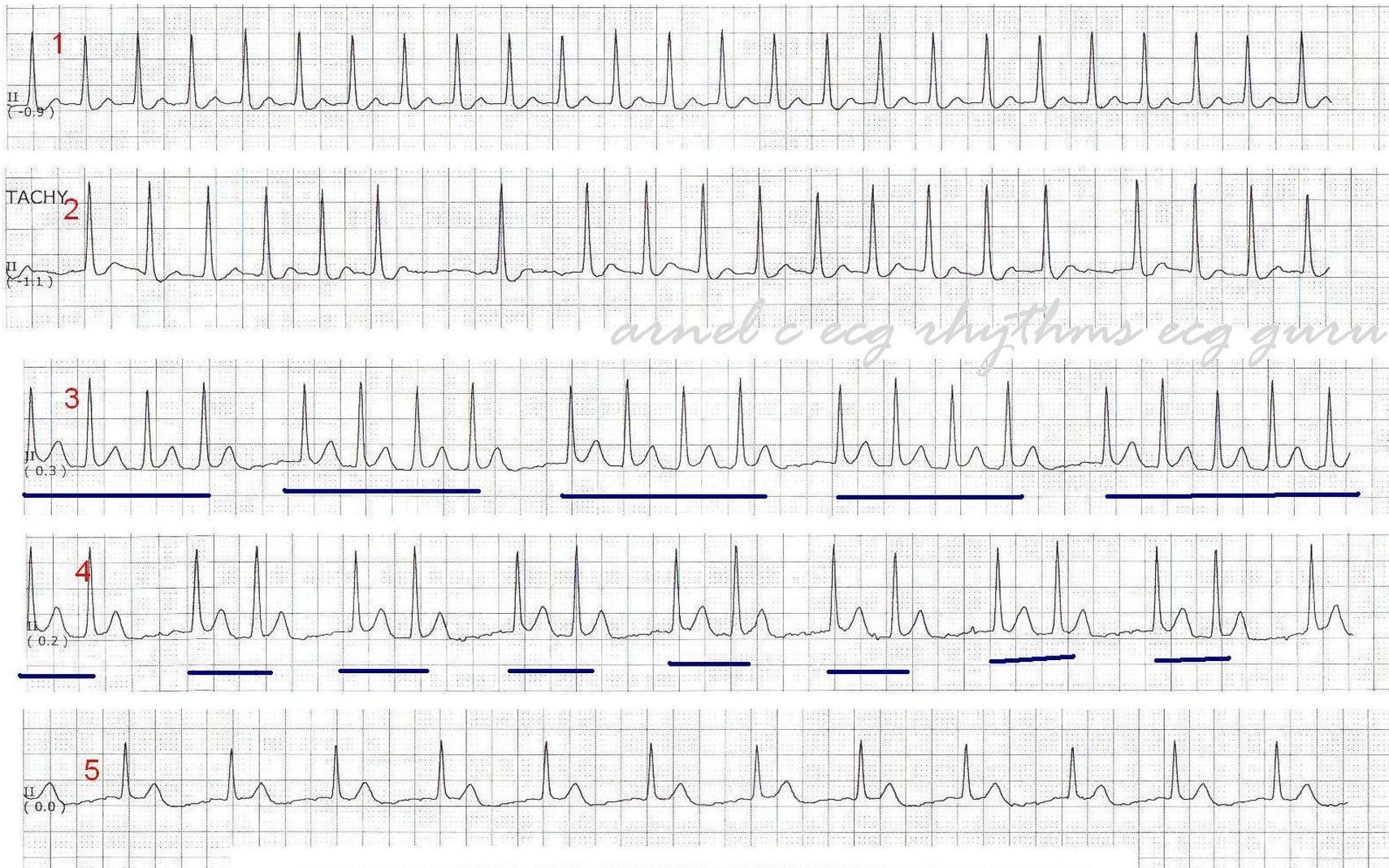
Strip 1: Narrow-complex tachycardia with NO apparent P waves.
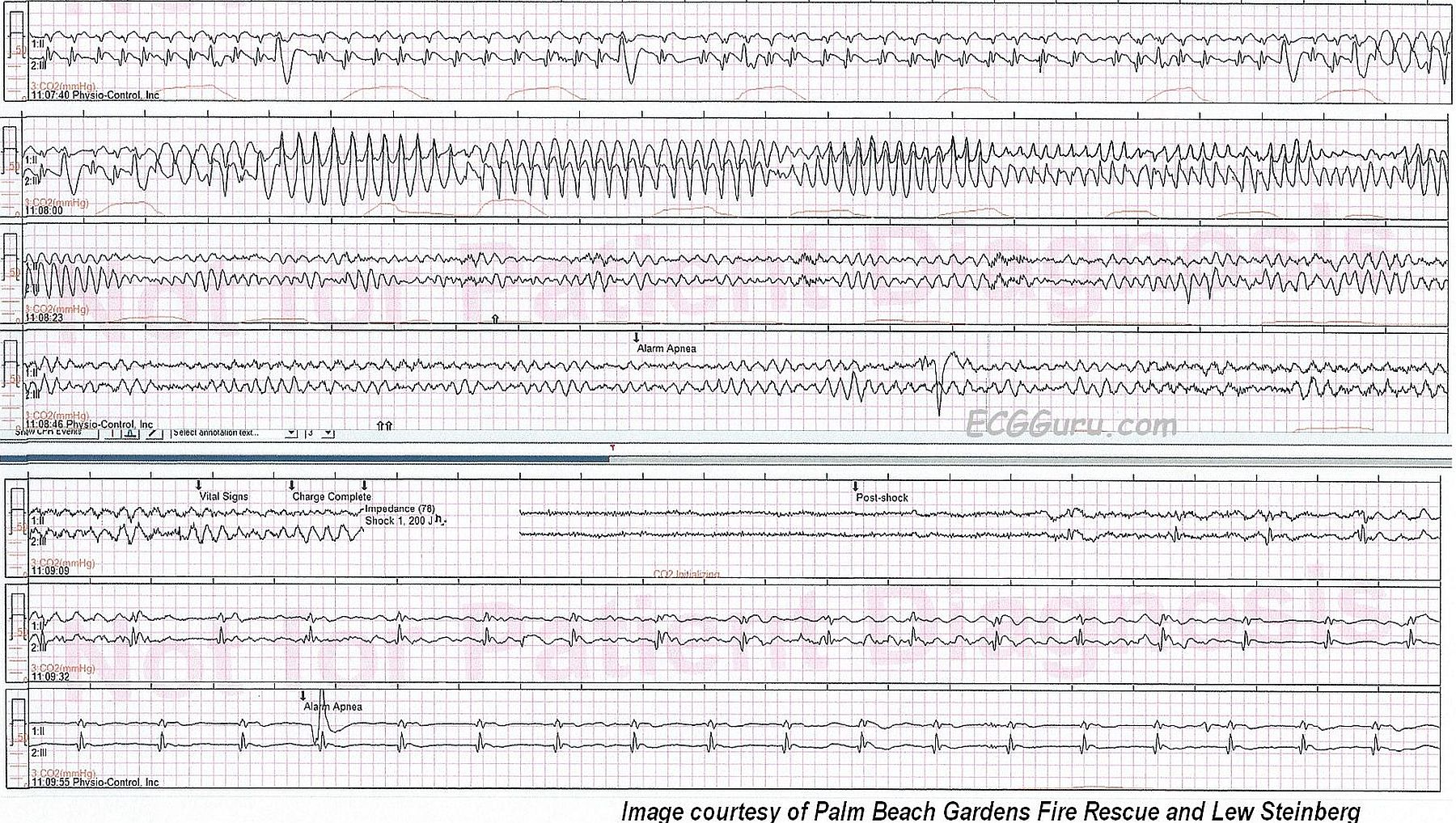
Strip 2: Some irregularity, with long regular groups and still NO P waves.
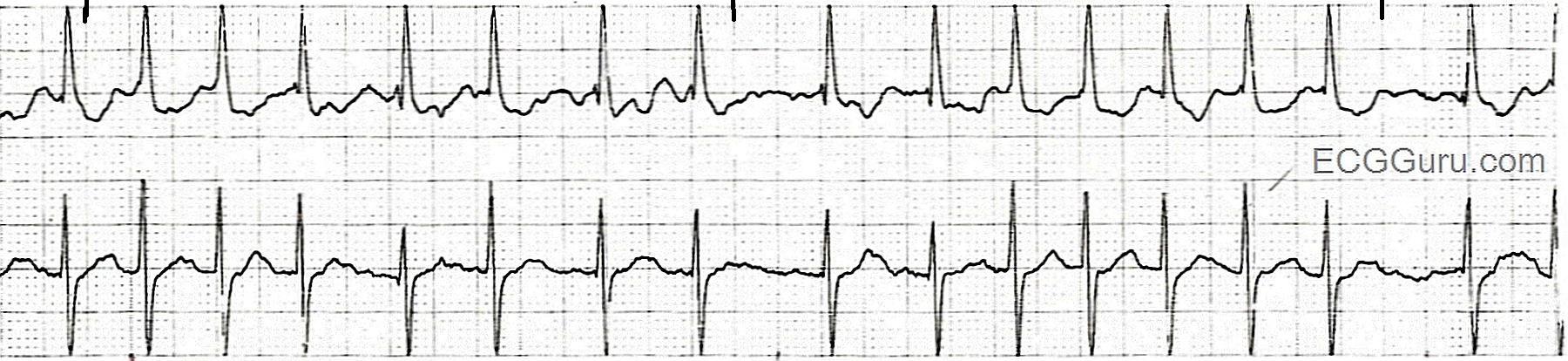
Strips 3 & 4: Grouped beating.
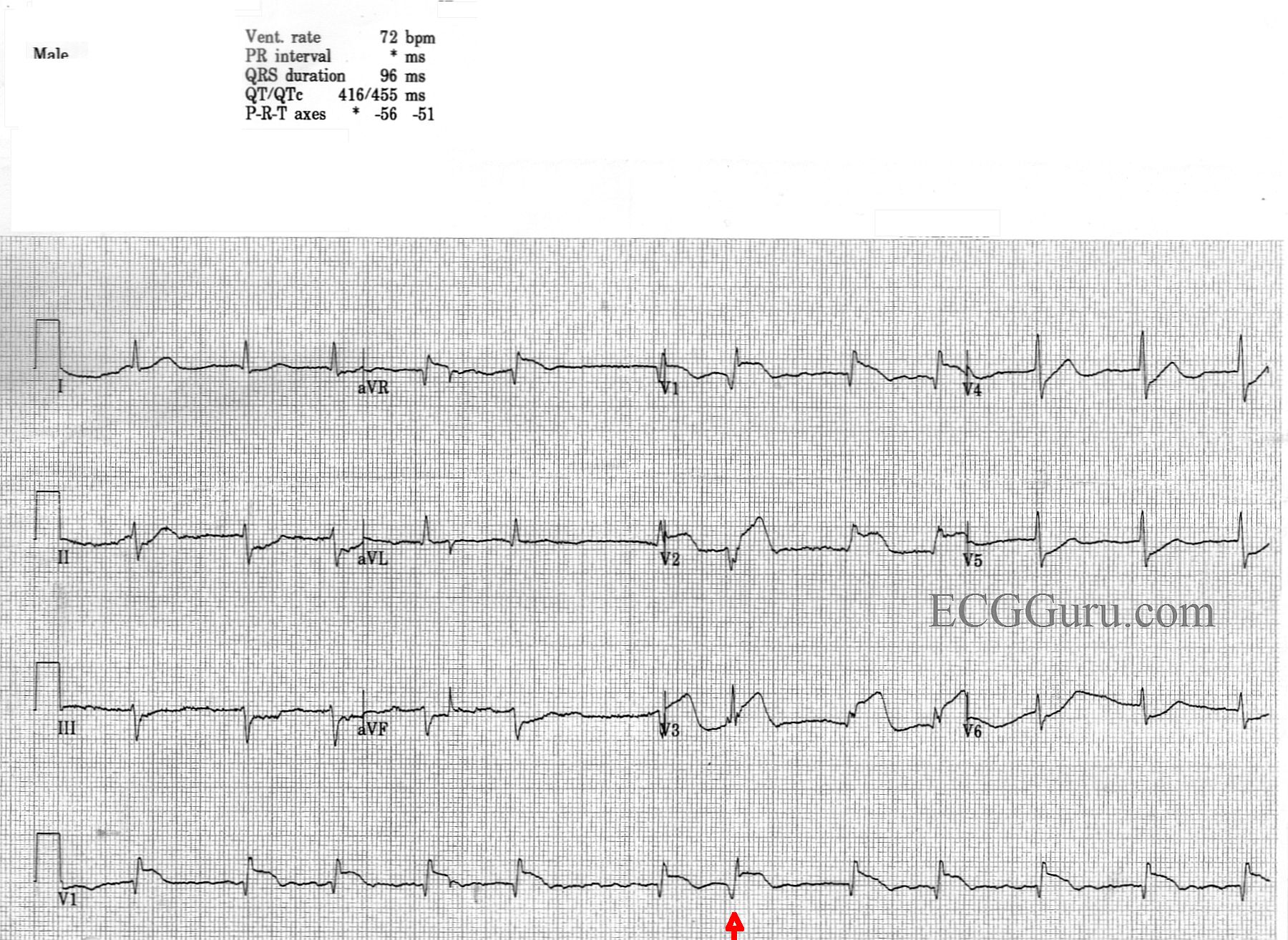
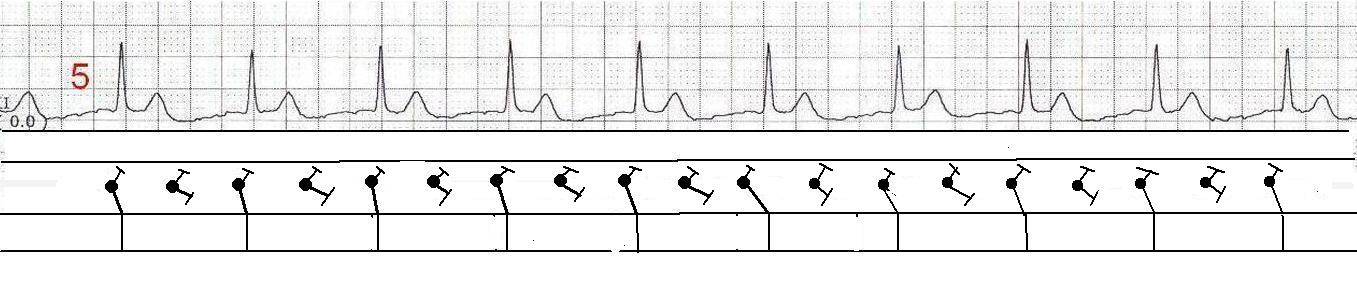
Strip 5: A narrow-complex rhythm that is approximately ½ the rate of Strip 1.
When grouped beating is seen, one should always suspect Wenckebach conduction. Wenckebach conduction (progressively longer conduction times through the A-V conduction system) can occur in rhythyms other than sinus rhythm. Without P waves and PR intervals, GROUPED BEATING is our major clue to Wenckebach conduction.
This patient has an underlying atrial fibrillation – hence no P waves. Fine fibrillatory waves can be seen, but artifact can cause the same appearance. So, why is there no irregular irregularity? There is another rhythm at work here along with the atrial fibrillation. Junctional tachycardia is seen in Strip 1. When two tachycardias coexist, one from above the AV junction, and one from below, the rhythm can be called a “double tachycardia”. This particular combination often happens in patients with digitalis toxicity.
In some cases, a complete heart block at the level of the atrial conduction fibers or the AV node causes two rhythms to operate independently. Any supraventricular rhythm, including atrial fib, can occur with a complete heart block, in which case we would see an “escape” rhythm. Escape rhythms are usually slow, either idiojunctional (40-60 bpm) or idioventricular (< 40 bpm).
Let’s look at each of the strips in detail. We will begin with the hypothesis that this is atrial fibrillation with concurrent junctional tachycardia at around 150 bpm. I will include laddergrams to illustrate my view of what is happening.