Submitted by Dr A Röschl on Tue, 01/14/2025 - 01:53
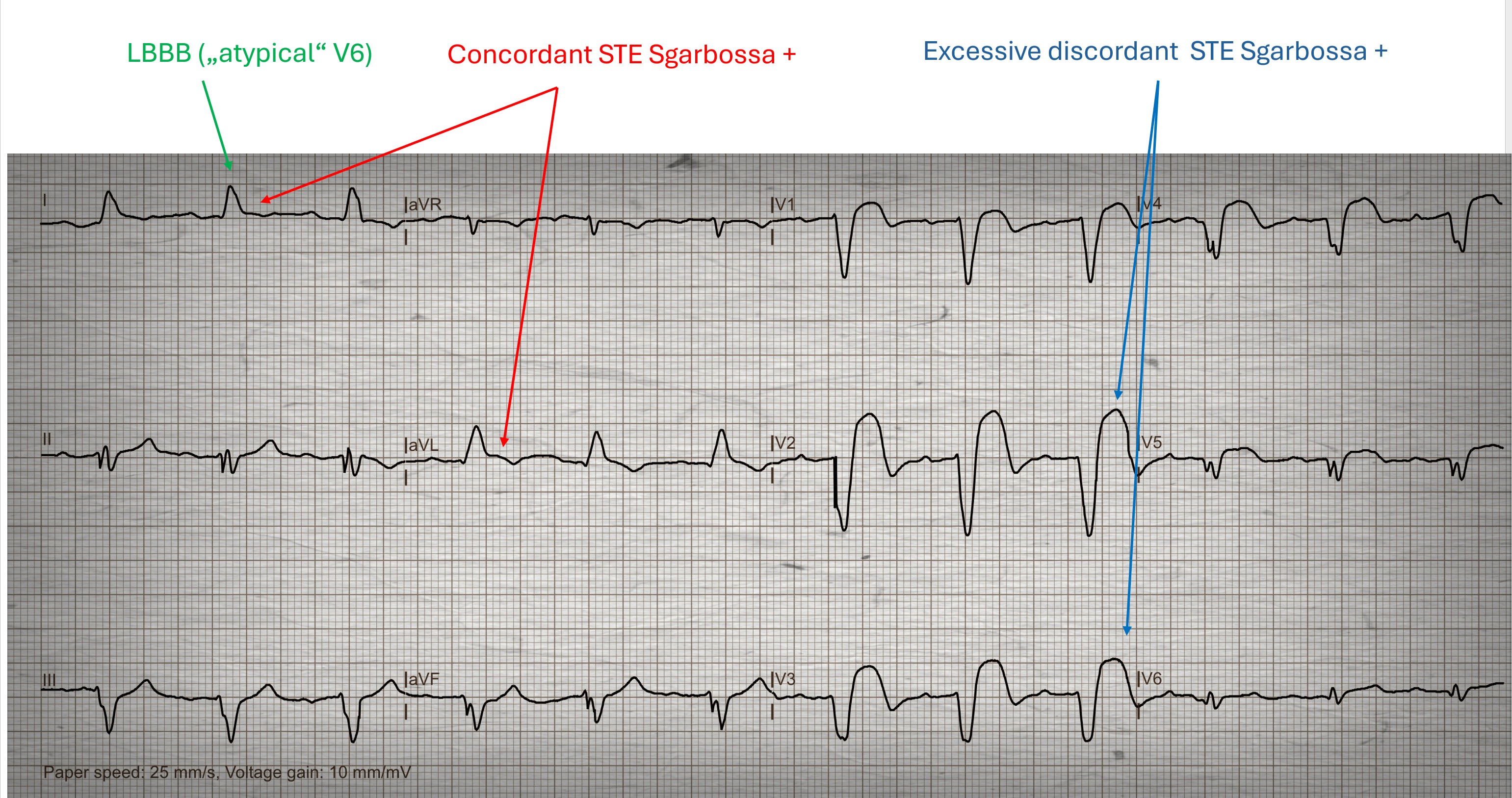
This ECG was sent to me by a friend, I don't know if he did it himself. The question was whether a heart attack can be recognized here. The patient is a 55-year-old man who has typical angina pectoris lasting more than 1 hour.
What can you answer?
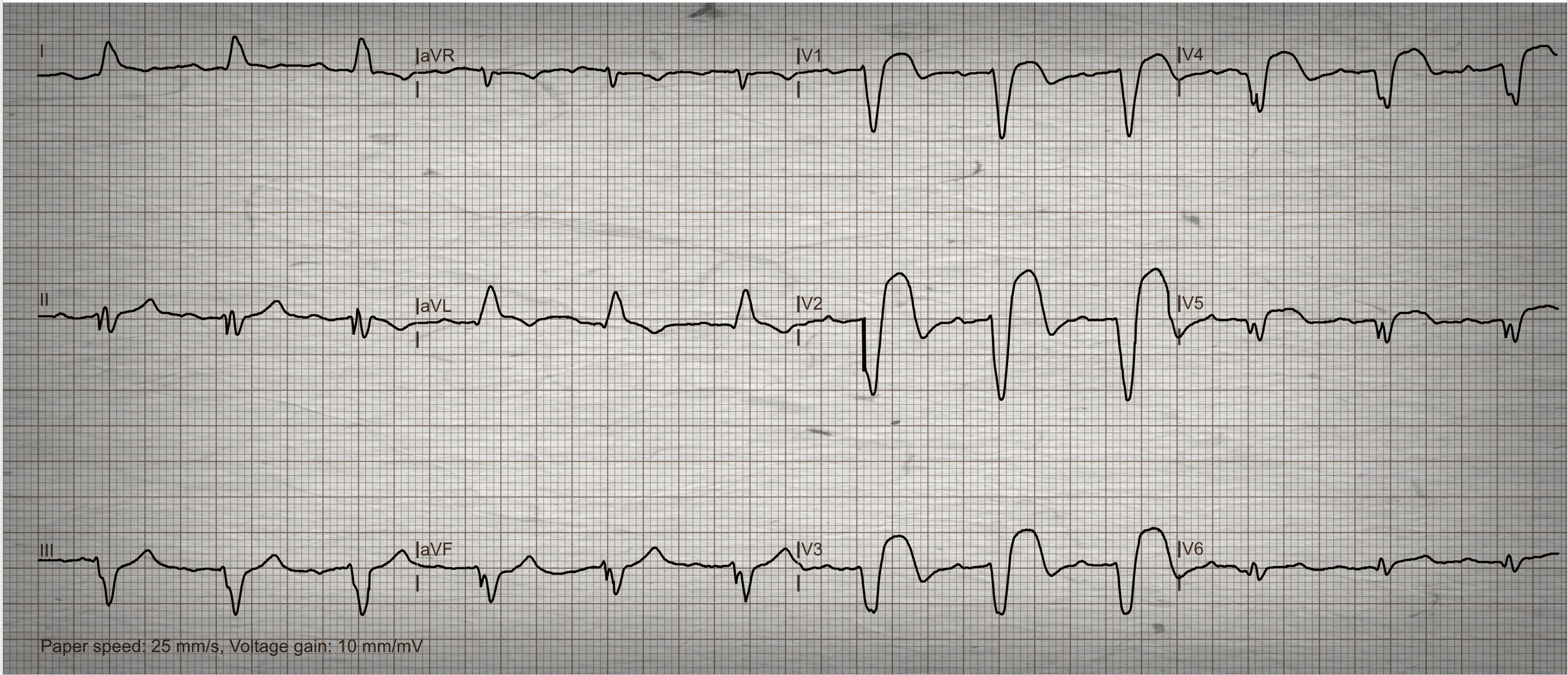
The Patient:A 64-year-old man complaining of chest pain and shortness of breath for 20 minutes.Long-standing history of triple vessel disease, severe aortic stenosis, hypertension, thrombocytopenia.Meds unknown.He was not considered to be a candidate for valve surgery.
The ECG: There is normal sinus rhythm with a rate of 90 bpm.P waves are not visualized well in all leads, so remember that the three channels of this ECG are run simultaneously.If you see a P wave in Leads I and II, they are also present in Lead III.The PR interval is WNL.
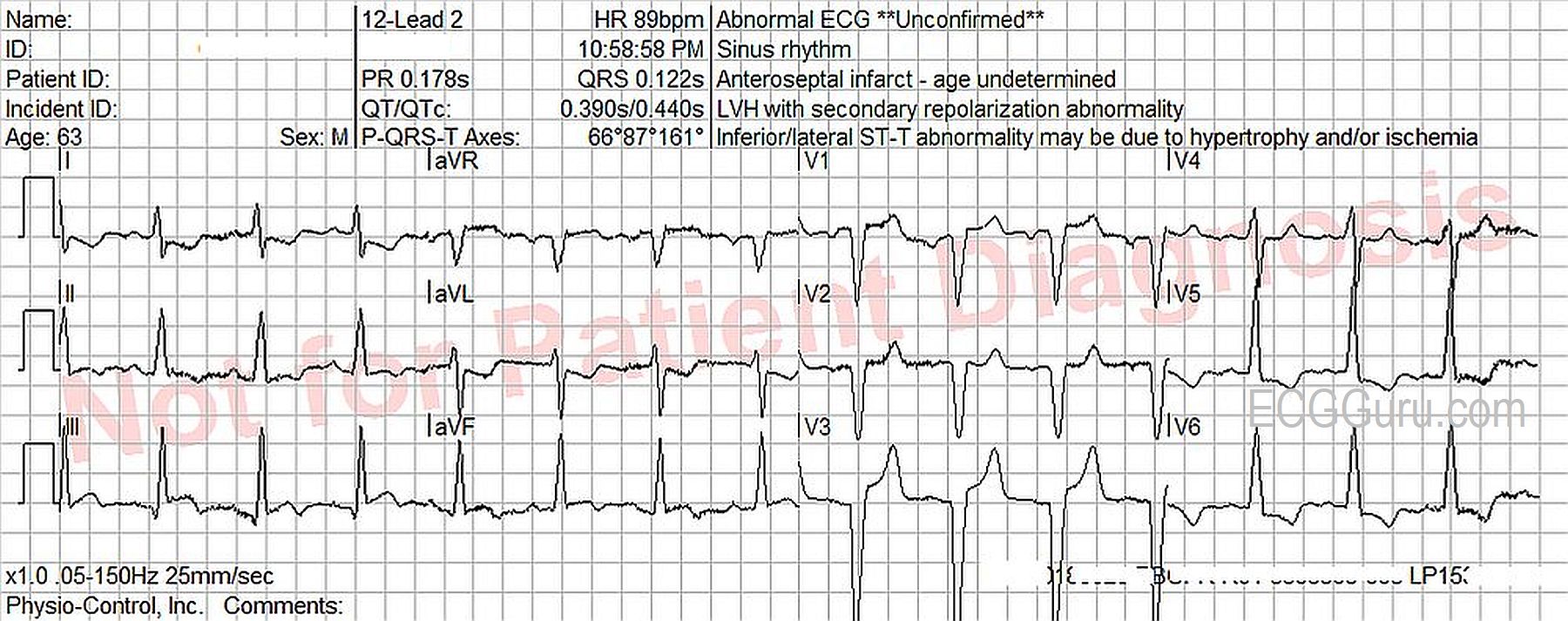
The QRS complexes are wide, at .122 seconds (122 ms).The criteria for left bundle branchblock are met. (Supraventricular rhythm, wide QRS, upright QRS in Leads I and V6, negative QRS in V1).The frontal plane axis is within normal limits, but toward the right, at 87 degrees.The QRS complexes transition at V4 from negative to positive, but Leads V1 – V3 have no initial r waves.These are possibly pathological Q waves, likely from a past anterior-septal M.I.
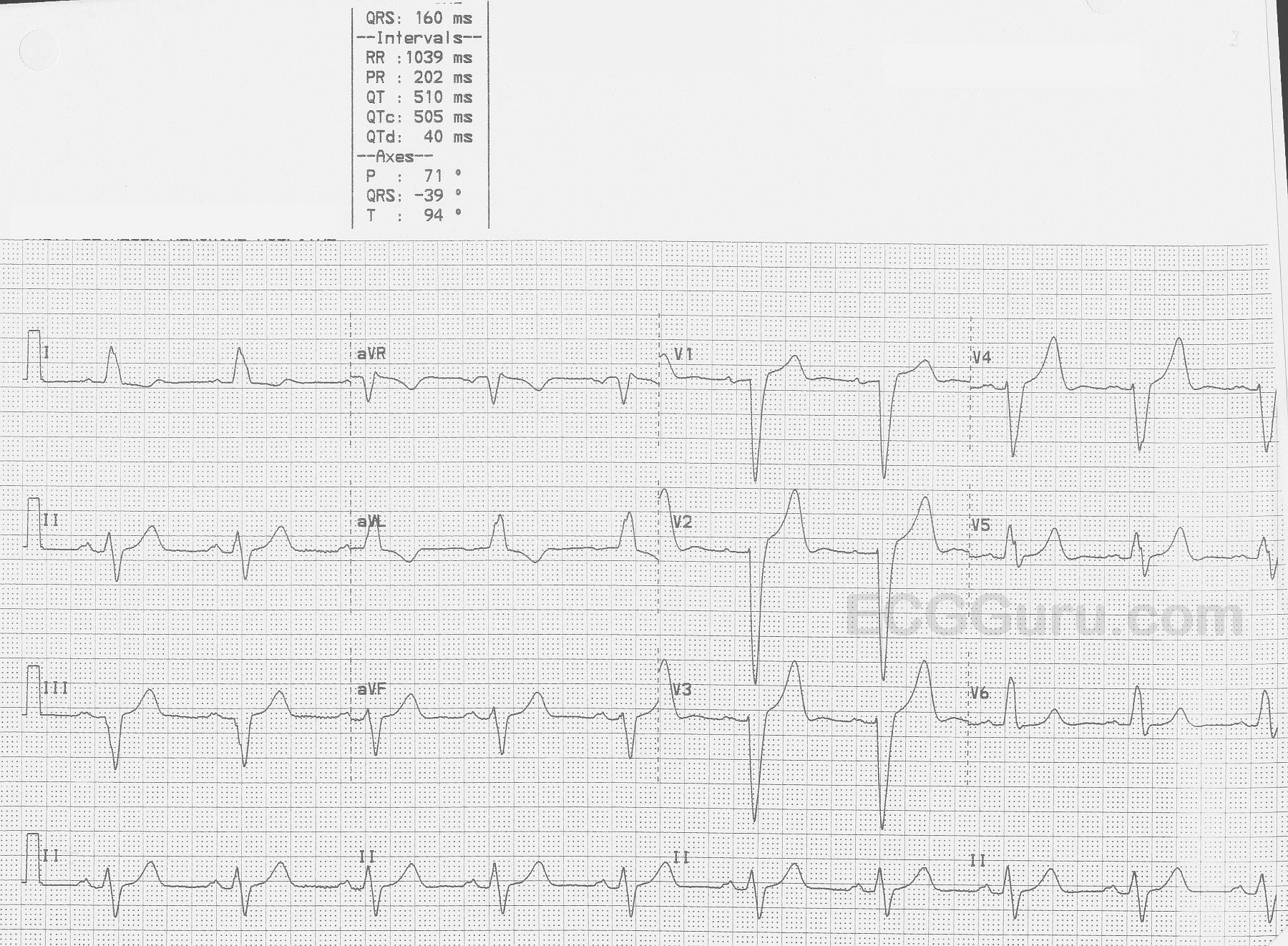
This ECG is taken from an elderly man with heart failure.
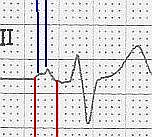
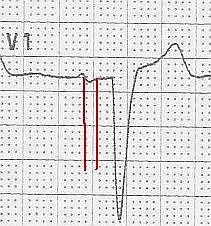
The ECG The first feature that might capture your attention is the wider-than-normal QRS complex, which is 160 ms (.16 seconds).The rate is 58 bpm. We do not know the patient’s medications or baseline rate.There are P waves present, and so the rhythm is SINUS BRADYCARDIA. The P waves are broad , > 110 ms in Lead II (red lines in close up) and bifid, with greater than 40 ms between the two peaks in Lead II (blue lines).In V1, the P waves are biphasic, with the terminal negative portion greater than 40 ms duration (red lines). This meets the ECG criteria for LEFT ATRIAL ENLARGEMENT, or preferably, LEFT ATRIAL ABNORMALITY. (https://LITFL.com/left-atrial-enlargement-ecg-library/) ECG criteria are not highly accurate for detecting atrial enlargement, and abnormal findings should be confirmed by anatomic measurement. (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2244611/).
The QRS complexes, as mentioned, are wide. Because there is sinus rhythm, we know the delay in conduction is due to interventricular conduction delay, and not to ventricular rhythm.This ECG meets the criteria for LEFT BUNDLE BRANCH BLOCK.