The Patient: Sixty-year-old man with a complaint of severe substernal chest pain. Denies hx of M.I., but reports feeling short of breath on exertion for about a year. Hx of hypertension, but admits he is non-compliant with his medication. Appears pale and diaphoretic, BP 110/68.
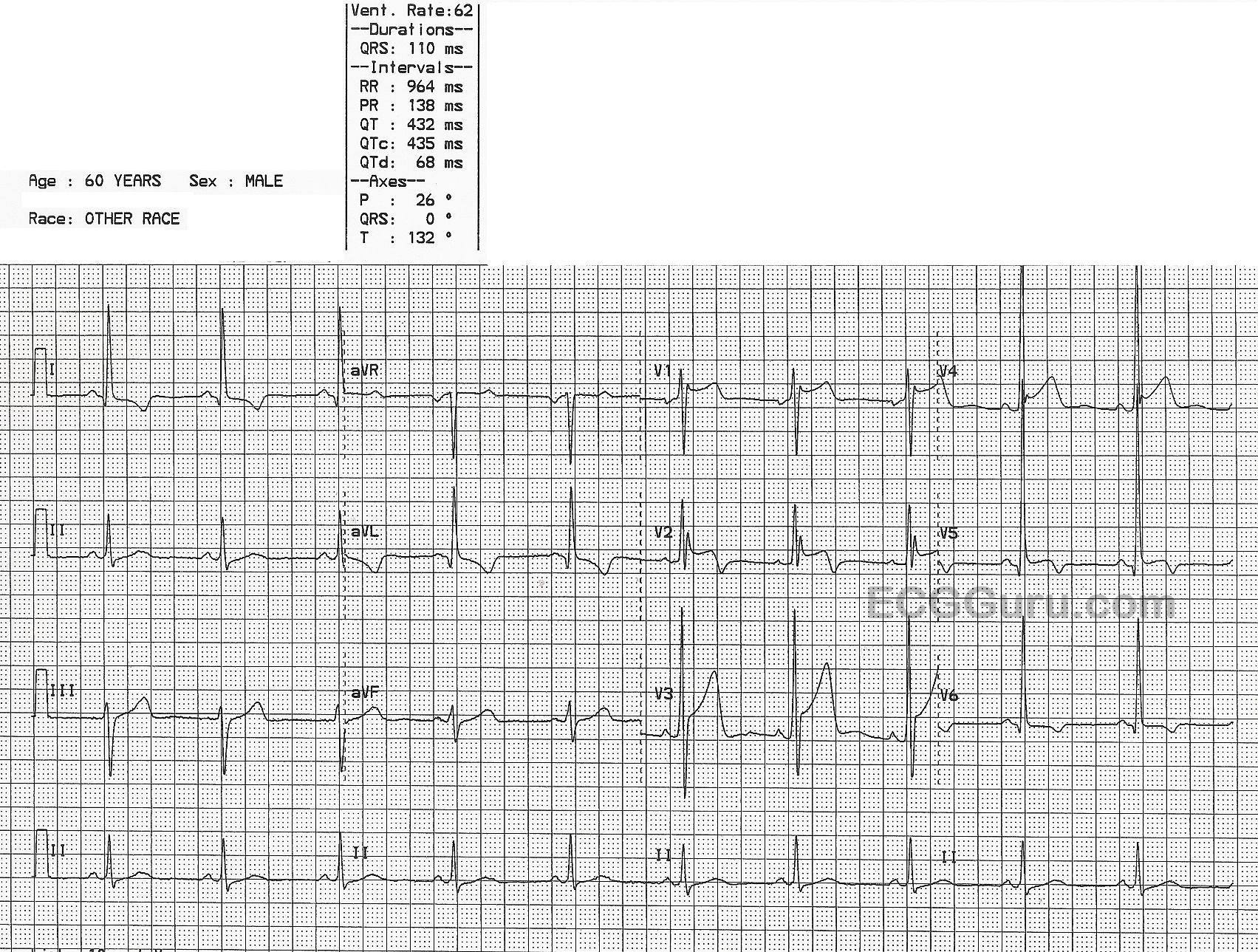
The ECG: The rhythm is sinus at 62 bpm. The QRS is slightly wide at 110 ms (.11 seconds), but still within normal limits. The intervals are WNL. The frontal plane axis is slightly leftward, while still normal. The QRS complexes are tall, especially on the left side. The voltage meets criteria for left ventricular hypertrophy (LVH). This is also called left ventricular enlargement (LVE). There are several accepted criteria for determining LVH, and this ECG meets them all. The V1 S wave plus the V5 R wave equal 52 or 52 mm. There is a slightly increased R wave peak time in V5 and V6 (normal is about one small block). There is ST depression and T wave inversion in the lateral leads: I, aVL, V6. This is called the "strain" pattern. V5 is also a lateral lead, but something else is preventing ST depression.
Note the ST elevation in V1 through V5. This is acute transmural ischemia, or ST elevation M.I. The STE in V5 was enough to overcome the STD caused by the LVH. The more modern term for these ECG changes is “OMI”, or occlusion myocardial infarction . https://litfl.com/omi-replacing-the-stemi-misnomer/ This term replaces "STEMI", as it includes myocarial injury with ST elevation and also with other ECG findings that are classified as "STEMI Equivalents".
We don't have information regarding the patient's outcome, but it is worth mentioning that the BP of 110/68 is probably low for him, and he has poor peripheral perfusion, evidenced by his pale skin and sweating.