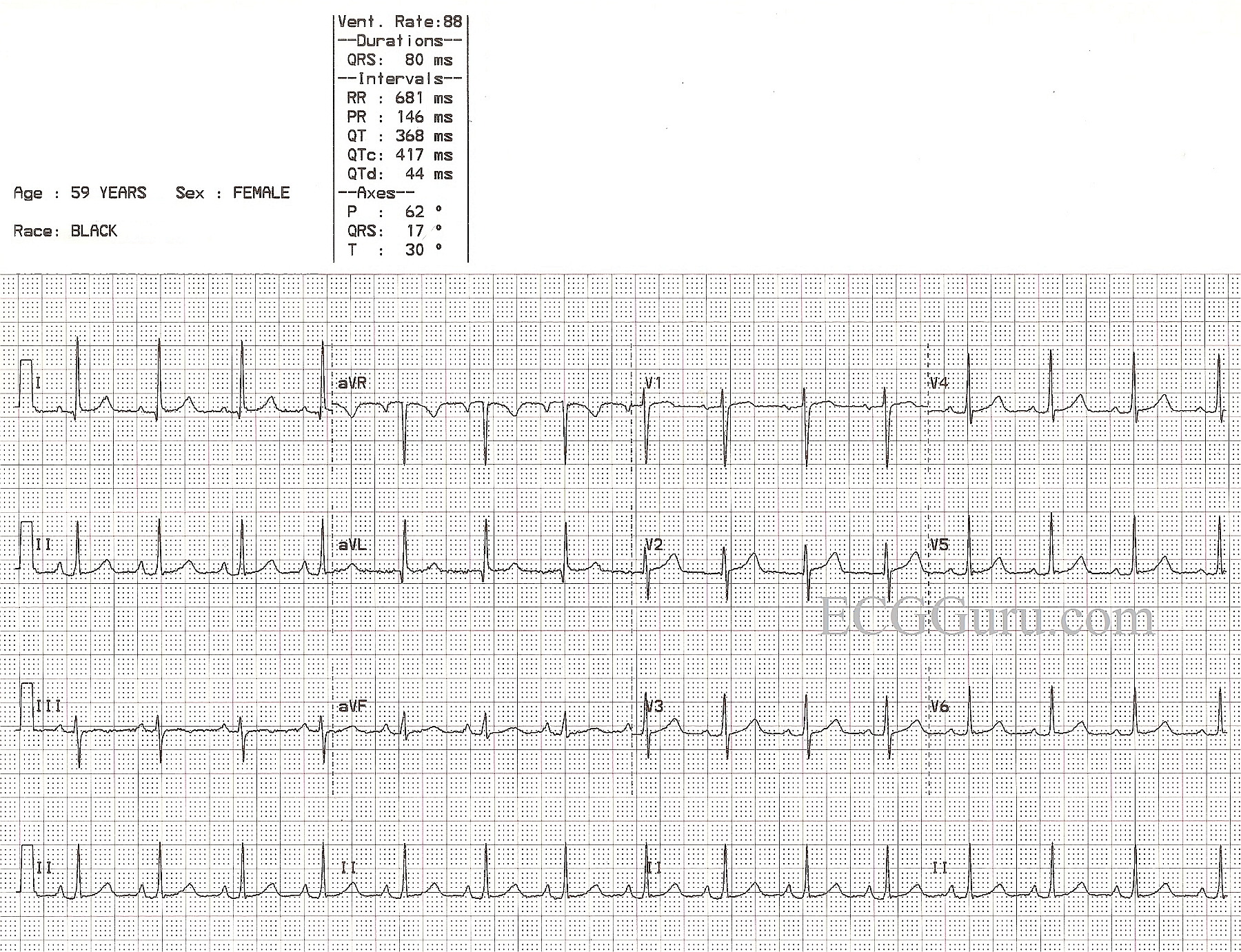
This ECG is nearly completely normal. We say "nearly" because there are VERY subtle changes which may or may not be chronic. Unfortunately, we know nothing about this patient's history or circumstances except age, gender, and race, and the fact that she was an Emergency Department patient. If she presented with chest pain, the ECG might be viewed completely differently than if she presented with a fever.
So, first, let's look at what is within NORMAL range. Most of these characteristics will be readily seen by your BASIC LEVEL students. The rate and intervals are within normal ranges. The rhythm is normal sinus rhythm. There is good R wave progression in the precordial leads. That is, V1 is primarily negatively-deflected and V6 is positive, with Leads V2 through V5 gradually becoming more and more positive. The frontal plane axis is within normal range - Leads I and II are positive. This would be a suitable ECG to use when introducing beginning students to the 12-lead ECG.
As for what is NOT NORMAL, there are several subtle characteristics. First, the P waves are slightly tall and have a pointed appearance. The P wave in V1 is biphasic. This can represent P PULMONALE, a sign of right atrial strain. This is often seen with pulmonary disease. One might also expect to see a shift of the frontal plane axis to the right if there is right ventricular hypertrophy as a result of increased strain on the right heart, but here we see a subtle shift to the left. The axis is still within normal limits, but at 17 degrees, it is closer to the left than the right.
The ST segments here are not perfect. One could argue that there is VERY slight elevation in Leads I and aVL, and the shape of the ST in V1 is coved upward. Lead III's ST segment is flat, and the T wave is inverted. Without clinical corelation, it is impossible to determine the importance of these changes. It is a good discussion to have with your more advanced students.
As said, it would be MUCH easier to ascribe meaning to these changes if we knew something of the patient's chief complaint, symptoms, and history.