Submitted by Dr A Röschl on Sat, 08/05/2023 - 03:27
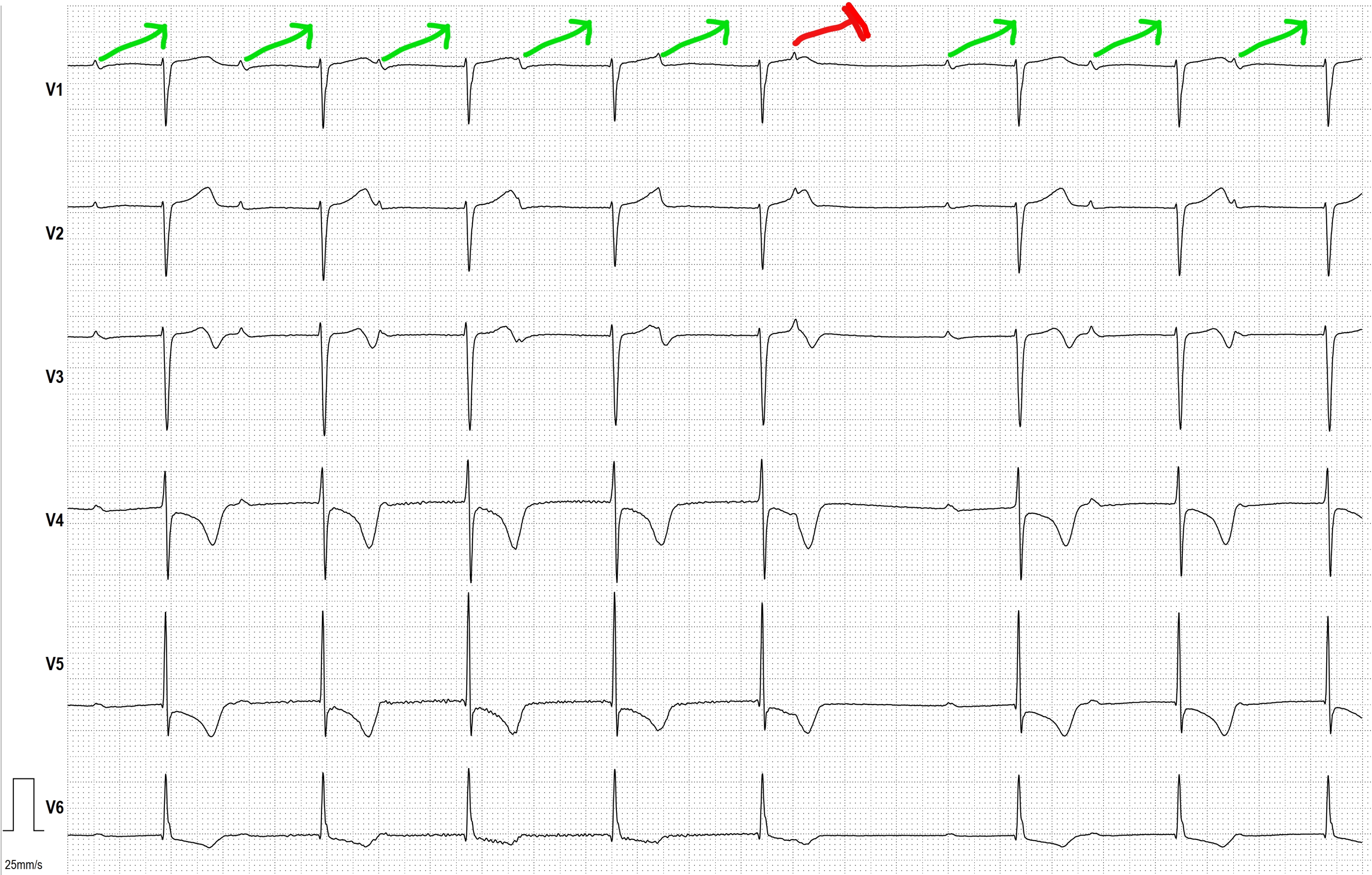
We see the EKG of an 81-year-old patient with a pacemaker; the PM was briefly deactivated to assess the patient's intrinsic heart rhythm. At the beginning of the EKG, there is already a prolonged AV conduction time, which progressively lengthens from beat to beat. The last conducted P-wave has a PR interval of nearly 800 ms (!). The next P-wave is blocked, but the subsequent displayed P-waves are conducted again, with the PR interval increasing from beat to beat. This indicates a classic second degree AVB Type Mobitz I (Wenckebach).