The Patient: A 60-year-old man at work. He experienced a sudden onset of substernal chest pain, nausea & vomiting, and dizziness. He states the pain is a 5 on 1-10 scale. No cardiac history or current medications.
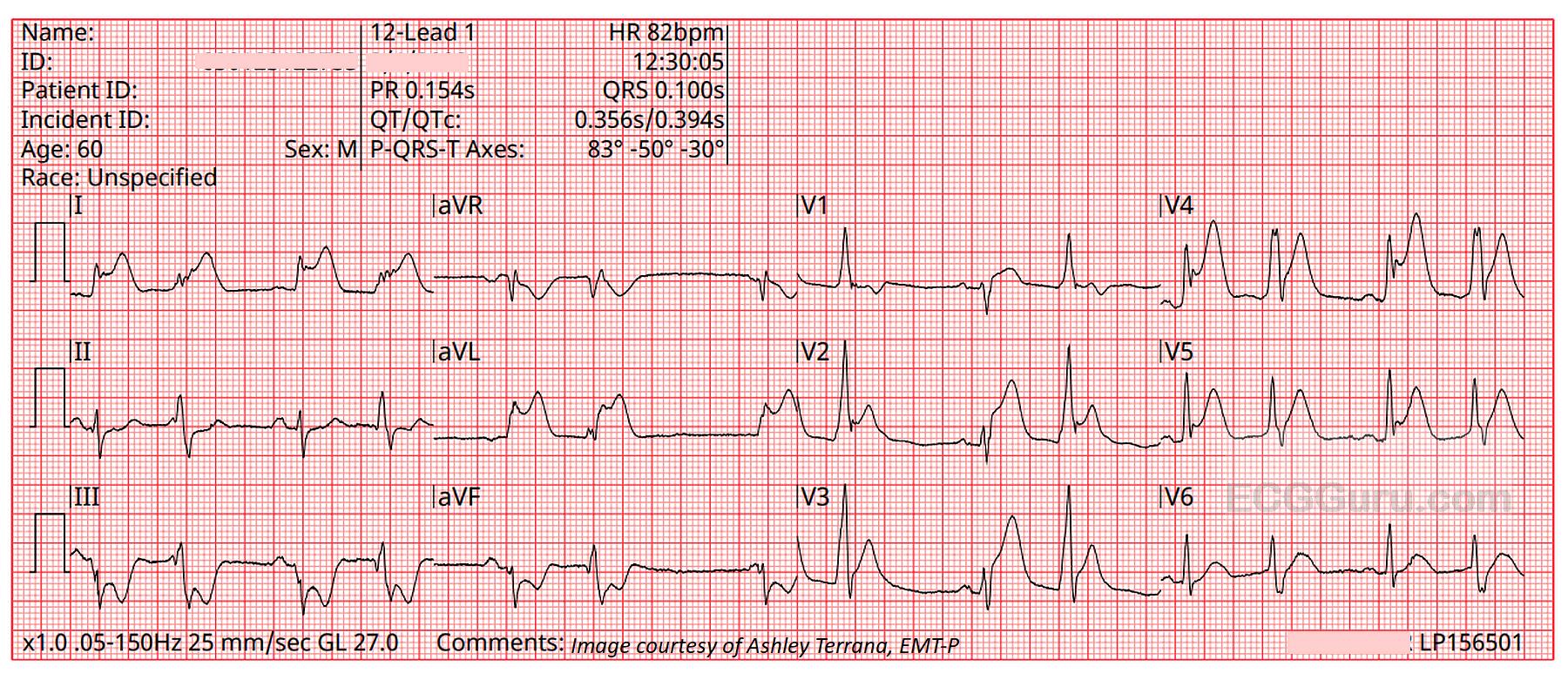
The ECGs: The first ECG, taken at 12:30:05, shows a sinus rhythm with ventricular bigeminy. In some leads, you can see the sinus P waves hidden in the beginnings of the PVCs, so we know the underlying sinus rhythm is about 82 bpm.
There is obvious ST elevation in V1 through V5, which is the anterior wall, an area perfused by the left anterior descending artery. Remember – the ST elevation sign may also show in the PVCs, but because ventricular beats have secondary ST changes of their own, we should assess only the sinus beats for ST changes.
There is also obvious ST elevation in Leads I and aVL. This is the high lateral wall, which is perfused by the circumflex and first diagonal arteries, both proximal branches of the left coronary artery. So, the involvement of the high lateral wall indicates a proximal lesion in the LCA – not good. Leads III and aVF have distinct ST depression – this is a reciprocal change reflecting the ST elevation in Leads I and aVL.