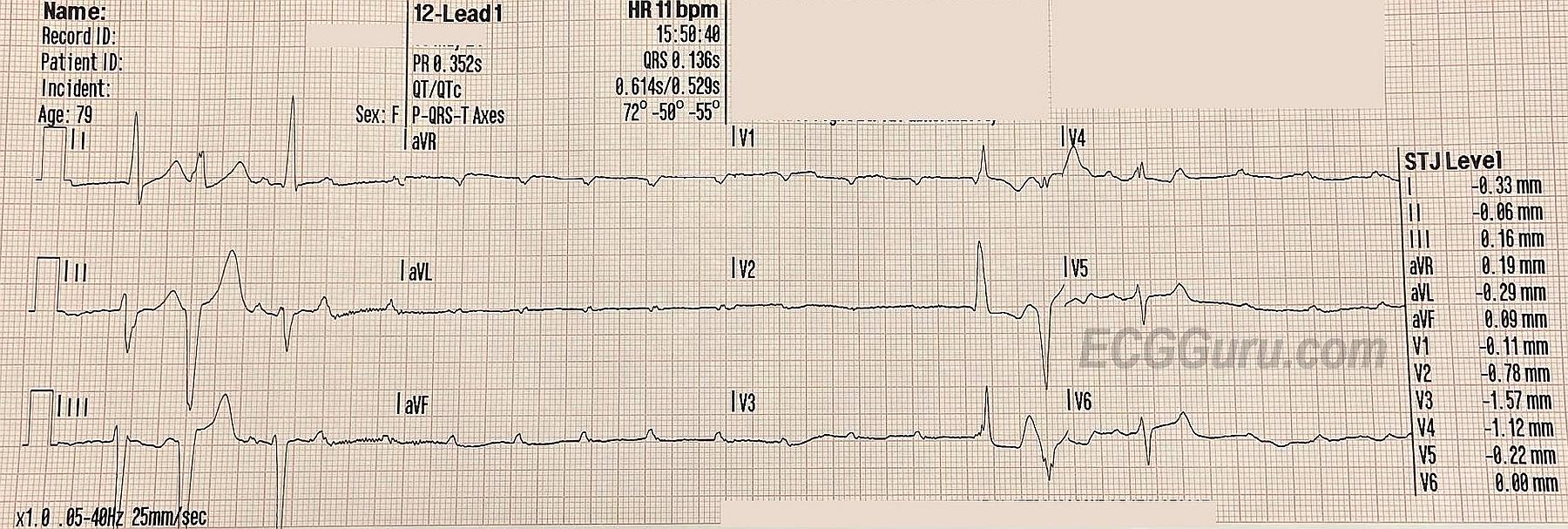
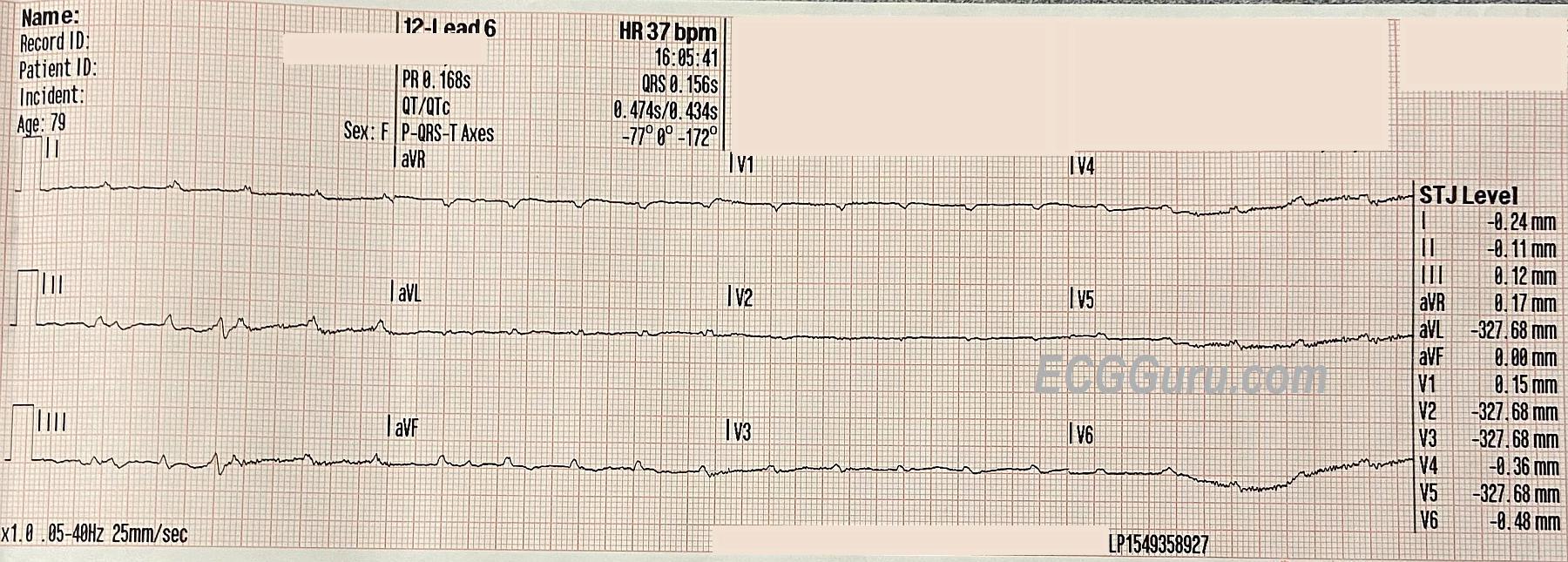
The Patient: This 72-year-old woman called EMS because of a sudden onset of breathlessness and anxiety. She had a history of COPD (asthma), CHF, and Type II diabetes. We do not know her medications or any other history. She was found to have bilateral breath sounds with "minimal" expiratory wheezing. She was alert and very anxious. Her initial pulse rate was recorded at around 60 bpm and irregular. A systolic BP was heard at 140 mm Hg, but the paramedic could not hear a pulse after that. She was given oxygen via CPAP (Continuous positive airway pressure). The first ECG at 15:50 was recorded during this assessment. After appearing to improve, she became neurologically altered, and her level of consciousness varied during the call. She was turned over to emergency department staff conscious and able to speak, but had a cardiac arrest subsequently. The paramedics were unable to obtain followup information regarding the outcome. ECG at 1550: The first QRS on the recording has no associated P wave, and is presumed to be an escape beat, probably junctional, with an interventricular conduction delay (QRS .12 sec.). This is a right bundle branch block pattern with left anterior fascicular block (bifascicular block). The second QRS is about the same width, but with a different morphology and discordant T waves, so probably ventricular. The third QRS is very much like the first, except that it appears to be conducted from the preceding P wave. For the next five seconds, there are only P waves, which are regular at about 130 bpm. The three-beat pattern seen at the beginning repeats itself near the end. This ECG shows evidence of severe conduction blocks. The wide QRS complexes indicate interventricular blocks. In this case, some are probably premature ventricular contractions and some are sinus beats with bifascicular block. Even more worrisome is the intermittent loss of AV conduction. This can be called "intermittent trifascicular block", or "intermittent ventricular standstill". This is not a "third-degree AV block", because there are signs of AV conduction, but it is very close. With two of the three main fasicles of the left bundle branch blocked initially, it only takes a block in the remaining fascicle to produce a complete lack of AV conduction. Of course, there are no pulses during the time of ventricular standstill. The really concerning part of this situation is the lack of an ESCAPE RHYTHM. This is a good time for a temporary pacemaker, either transcutaneous or, if available, transvenous. ECG at 1603: This ECG was obtained enroute to the hospital. The patient is once again alert and anxious. There is some artifact which hampers evaluation, but there are two P waves for every QRS complex. The atrial rate is about 120 bpm and the ventricular rate is about 60 bpm. The non-conducted P waves are buried in the T waves of the preceding beats.