The Patient This ECG was obtained from an 80-year-old man with a past medical history of hypertension, diabetes, chronic obstructive pulmonary disease, hyperlipidemia, chronic kidney disease, and heart failure with preserved ejection fraction (HFpEF).
He presented to the hospital with a complaint of shortness of breath, and was determined to have an exacerbation of his COPD in the setting of a viral infection. He was treated with breathing treatments and steroids, and was discharged home in improved condition.
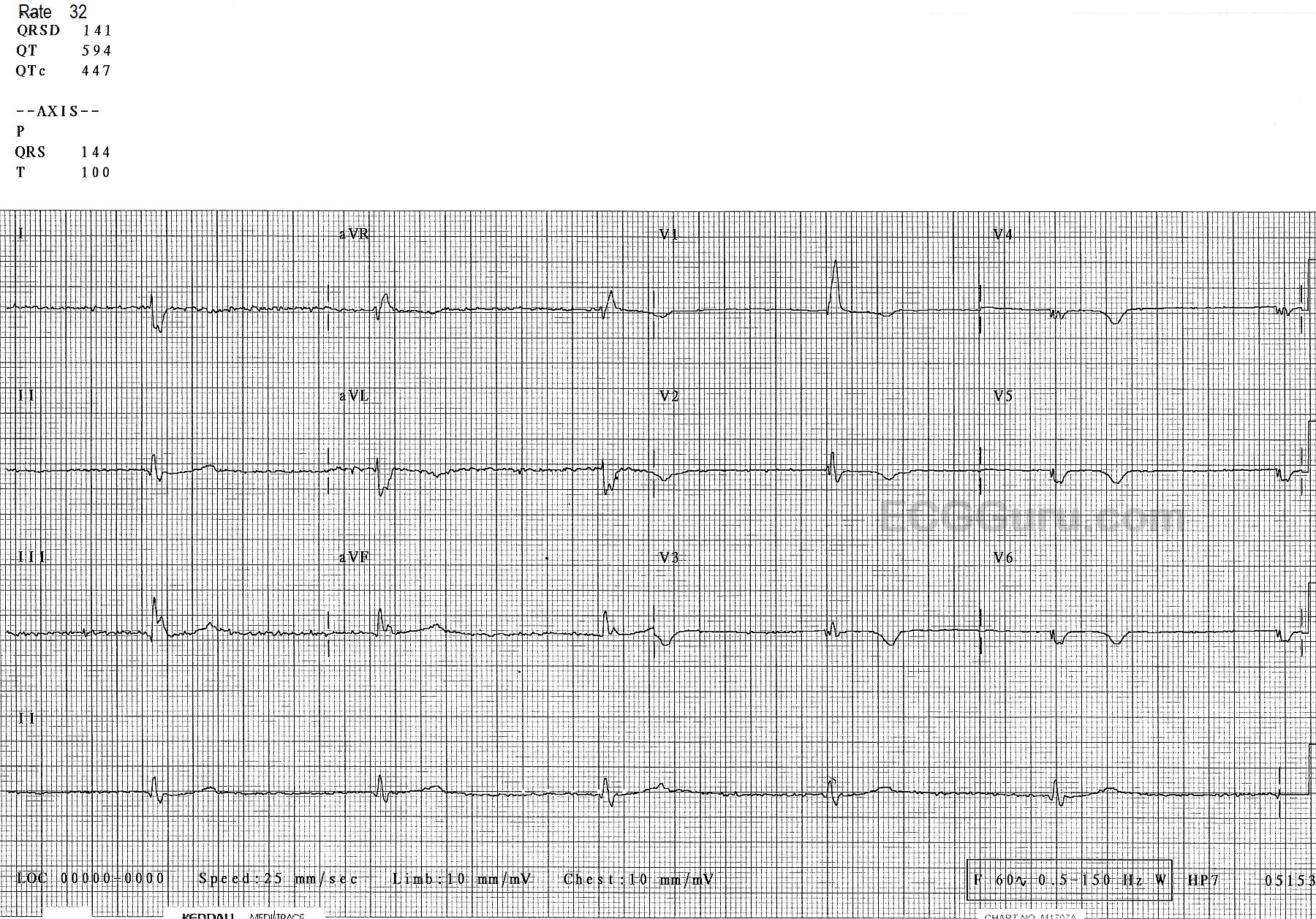
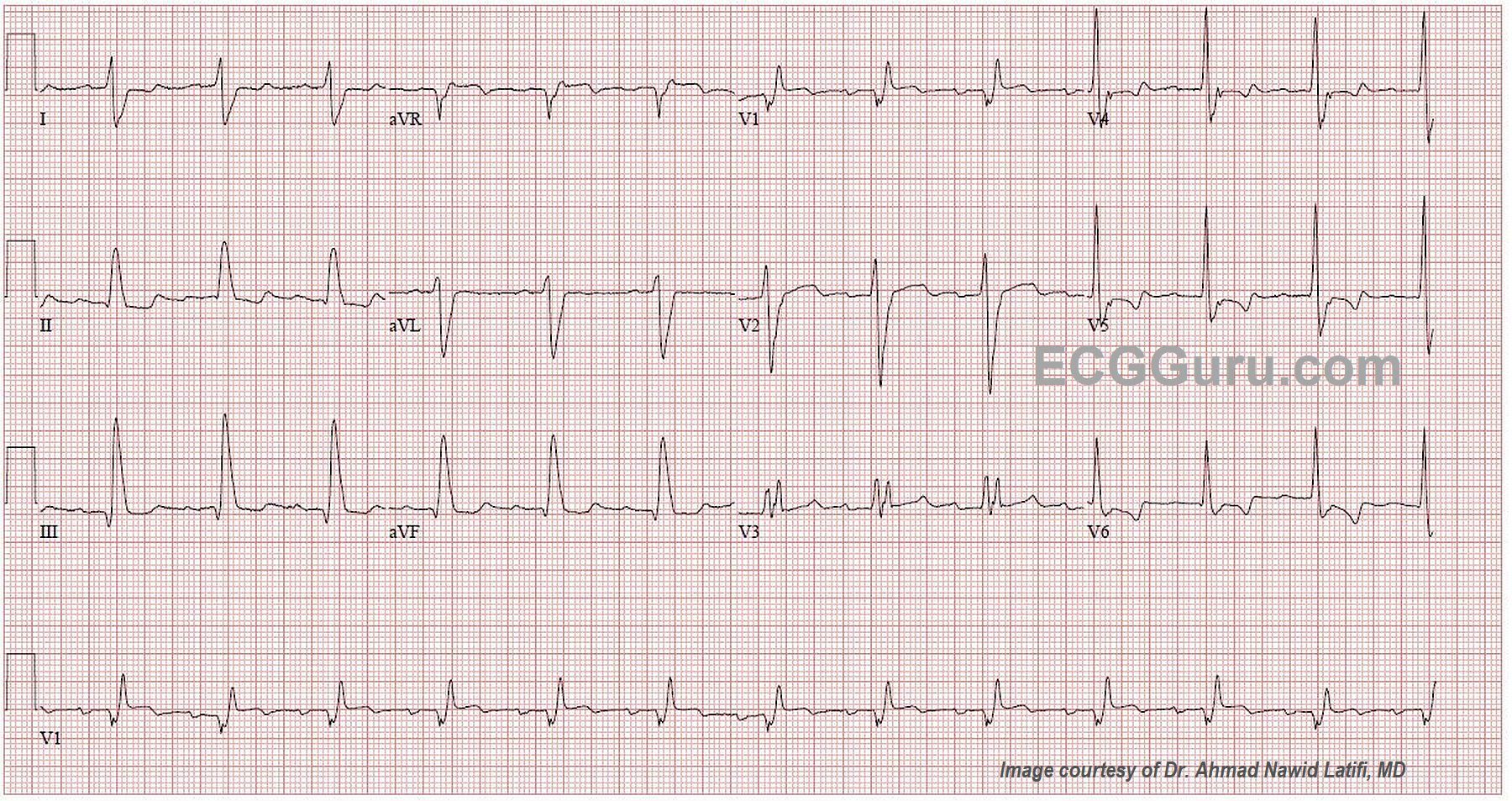
The ECG There is a sinus rhythm at 80 bpm. The QRS complex is wide at .18 seconds (180 ms). The PR interval is slightly prolonged at .24 seconds (240 ms), which is first-degree AV block. There is right bundle branch block (QR in V1 and rS in Leads I and V6 with a wide QRS). There is also a left posterior fascicular block (also called hemiblock), recognized by the right axis deviation (III is taller than aVF ). This is bi-fascicular block, which can be chronic or acute. There is very slight ST elevation with flattening in V1 and possibly V2. In RBBB, “normal” T waves are directed opposite the terminal wave of the QRS. V3 should, then, have inverted T waves. So, the upright T wave in this patient could be considered to be equivalent to an inversion in a normal ECG. V4 through V6 have biphasic T waves, which is not normal for RBBB. Because we do not have an old ECG, we don’t know which, if any, of these changes are chronic. With this patient’s past medical history, it is possible for any of them to be pre-existing.
I will admit that, when I first saw this ECG, the V1 rhythm strip at the bottom looked as though there were regular P waves at a rate of about 220-240, with one buried in each QRS and one in each T wave. In scrutinizing all the other leads, I cannot find evidence for an underlying atrial tachycardia or atrial flutter, so it is probably a coincidence that the P and T “march out” with the assumption of a hidden P wave in the QRS.