Wide-QRS rhythms can be difficult to diagnose from the ECG alone. This difficulty is compounded when the rate is fast, as it can be hard to determine if P waves are present before the QRSs, or dissociated, or absent.
This ECG and rhythm strip were donated to the ECG Guru by Ryan Cihowiak. We don't have clinical information on the patient, unfortunately. It is a great example, however, of how difficult WCT can be to diagnose.
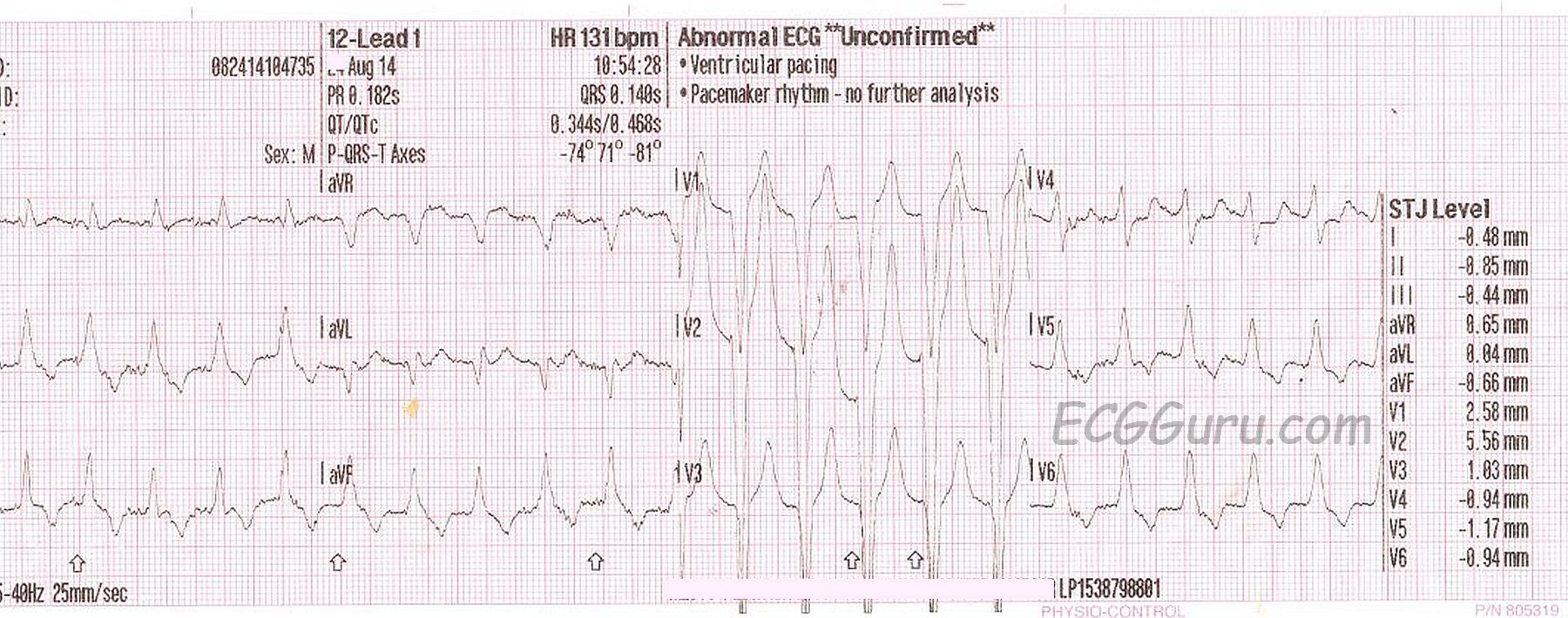
In the 12-Lead ECG, we see wide QRS complexes that are regular at a rate of 131 / minute. There are no obvious P waves before the QRS complexes, and no obvious distortion of the T waves, which would suggest a "hidden" P wave. Unfortunately, there is significant artifact, which makes searching for P waves difficult. The pattern overall suggests left bundle branch block, with the negative QRS in Lead V1 and positive QRS complexes in Leads I and V6. However, one requirement for the diagnosis of LBBB is a supraventricular rhythm, and P waves are the best indicator of that. An irregularly-irregular rhythm, indicating atrial fib, would also have made LBBB more likely. In typical LBBB, the frontal plane axis is usually left-normal or left. In this ECG, Lead III is taller than Lead I, putting the axis within normal range, but slightly rightward.
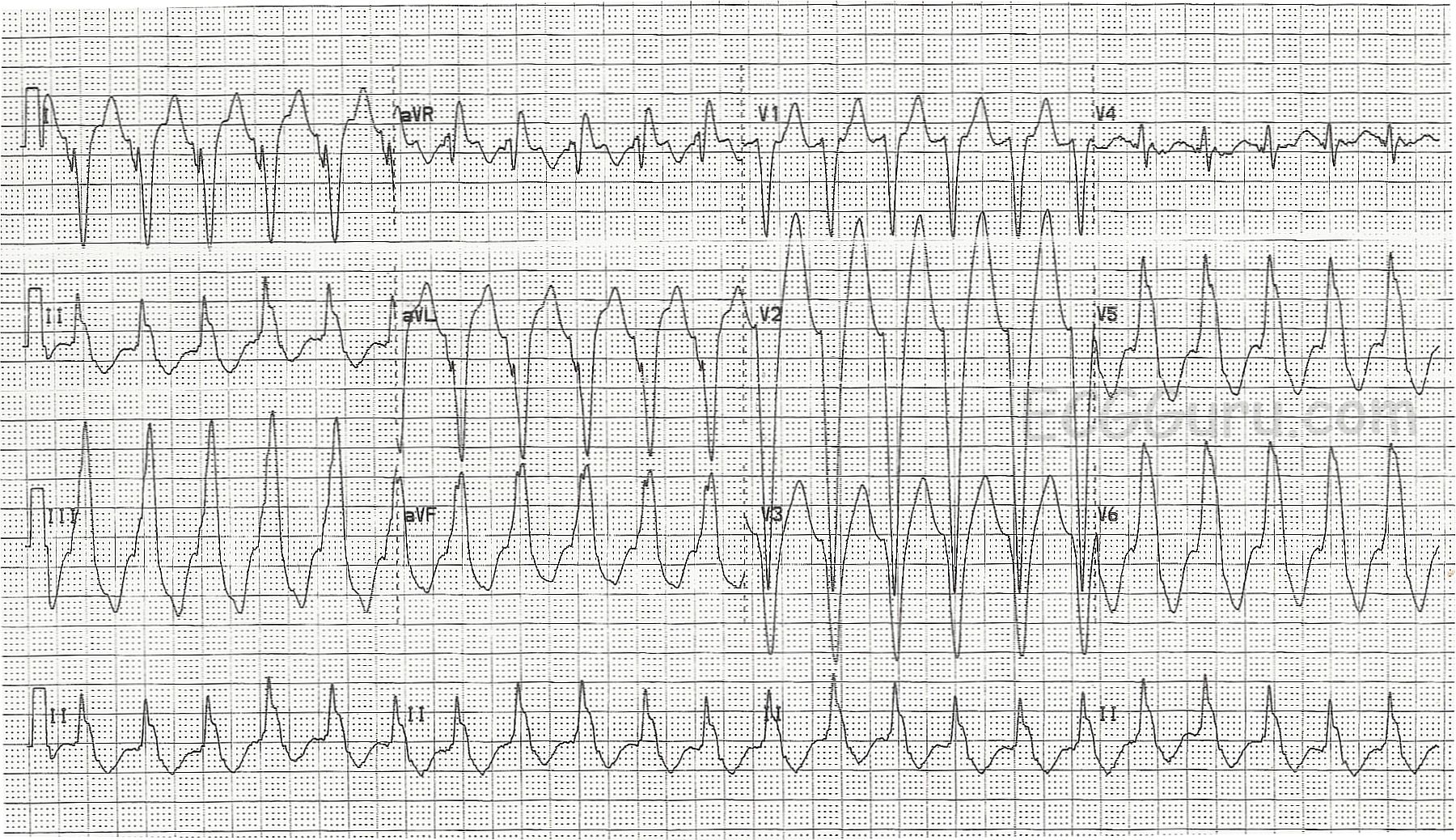
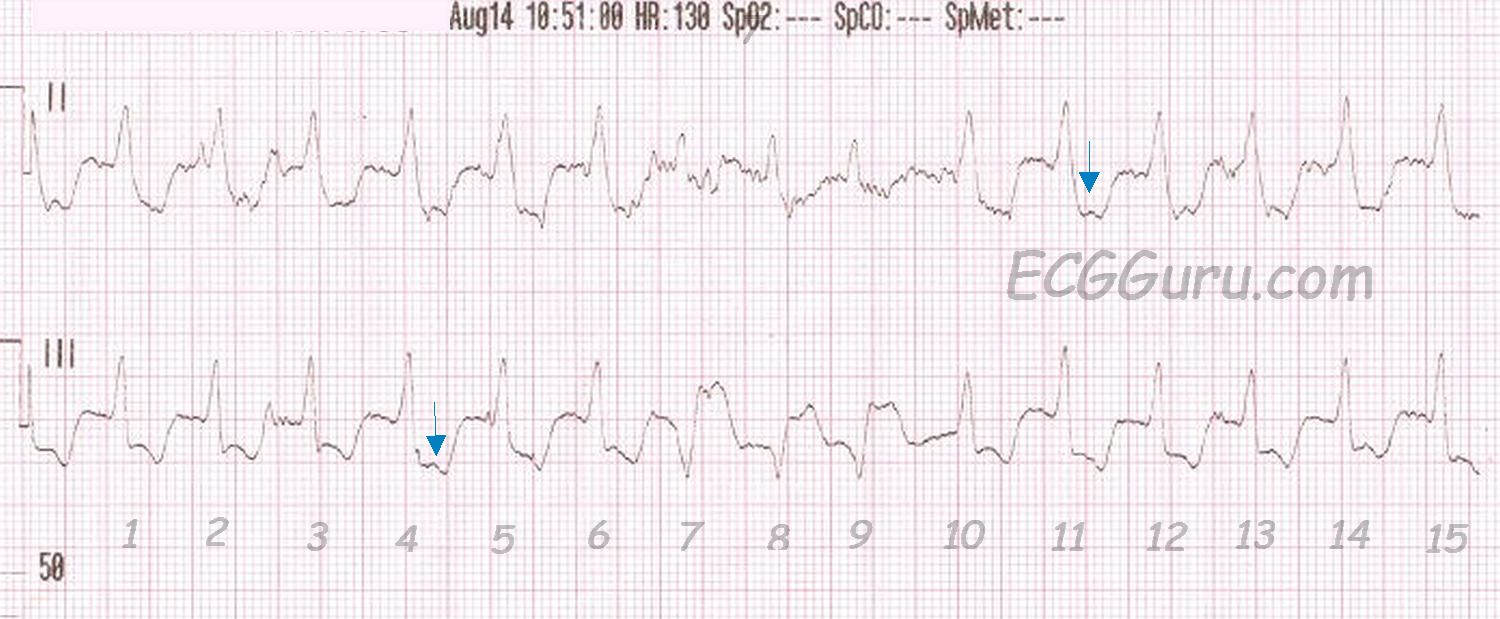
The rhythm strip uncovers something else. Possible P waves are seen in some of the ST segments (arrows). Are these dissociated? Do they represent a first-degree AV block? Are they actually artifact? If this is a supraventricular rhythm, there is LBBB. Then, notice beats #7,8,9. If this rhythm is supraventricular (with LBBB), those must be a salvo of V Tach. But, one of the possible P waves occurs in front of beat #7.
Another possibility is Right Ventricular Outflow Tract Tachycardia. RVOT is a type of V Tach that typically has a LBBB pattern, with a slightly rightward axis. If this is the case, beats #7,8,9 are probably "capture" beats or "fusion" beats. Capture and fusion beats "prove" that the underlying tachycardia is ventricular, since, by definition, capture and fusion represent a return to supraventricular control of the rhythm.