The patient: This ECG was taken from a 66-year-old man who was complaining of chest pain at rest. He had been previously diagnosed with lung cancer with metastases to his bones. The last ECG, taken one week ago, was normal.
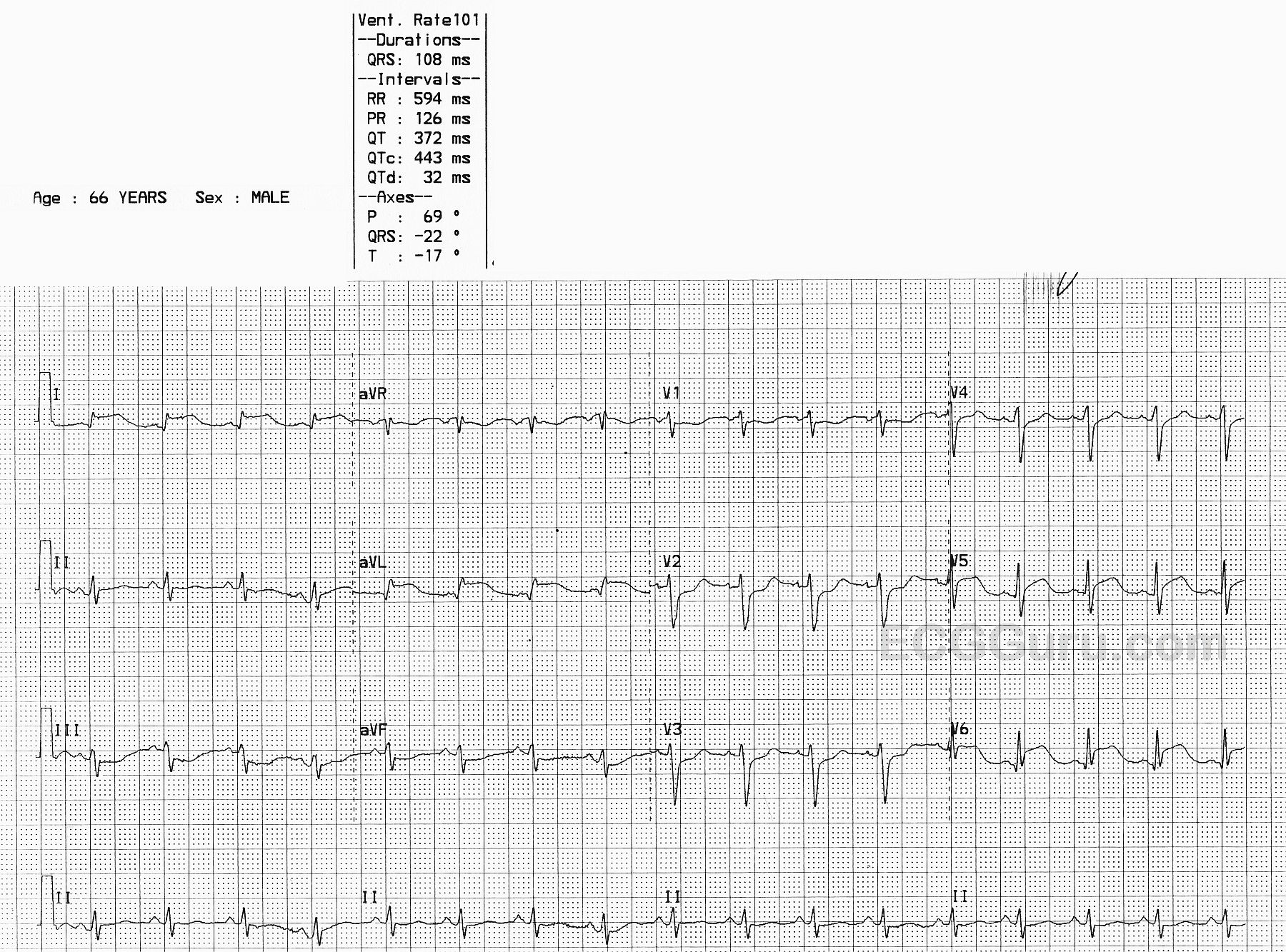
The ECG: There is mild sinus tachycardia at 101 bpm. The rhythm is regular. The QRS duration and PR interval are normal, as is the QTc. The QRS voltage in the limb leads is small, and we do not know the patient’s height and weight.
There are notable ST elevations in I and aVL (high lateral wall) and in V5 and V6 (low lateral wall). When the high and low lateral walls are similarly affected, we usually look to the circumflex artery as the culprit artery. We also see ST depression in Leads III and aVF (reciprocal to the STE in I and aVL) and in V1 – V4. This could indicate subendocardial damage or reciprocal changes. This ECG meets the criteria for acute lateral myocardial infarction.
The patient was taken to the cath lab emergently. His coronary arteries, including the left circumflex, all were free of occlusive lesions. He had no coronary spasm during the procedure, but it was decided that spasm had been the cause of the ECG changes. His ECG reverted to normal.
It is important to record abnormal findings, as some changes can be temporary or fleeting. Coronary artery spasm can cause ischemia and damage to the heart, just as plaque lesions and blood clots can.