The Patient: This series of ECGs is from a 65-year-old woman who was complaining of a sudden onset of chest pain, nausea, and weakness. She stated that the pain increased on inspiration. She reported a history of non-insulin-dependent diabetes mellitus (NIDDM).
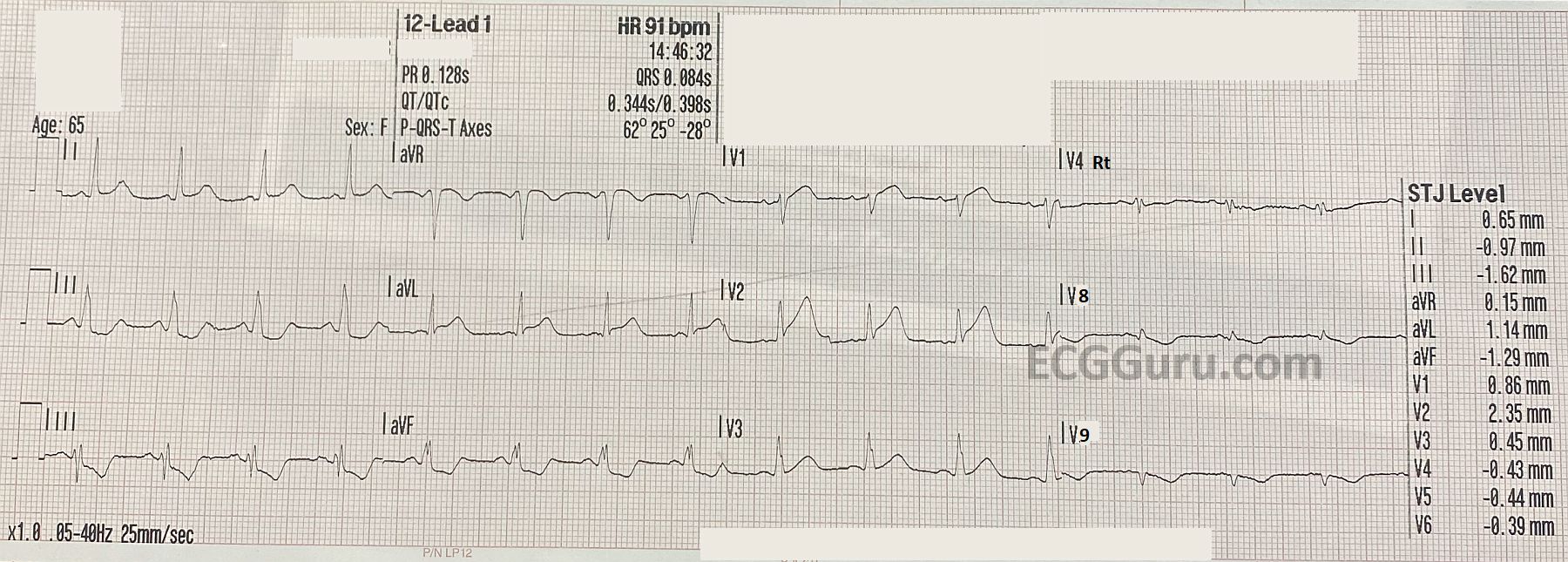
ECG No. 1, 14:46: This ECG includes V4Right, V8 and V9 in place of V4, V5, and V6. The rhythm is sinus at 91 beats per minute. The PR interval is within normal limits, as is the QRS duration. The QTc is WNL as well. The frontal plane axis is also WNL. The three standard chest leads show an early transition of R waves in V2. There are noticeable ST and T wave abnormalities:
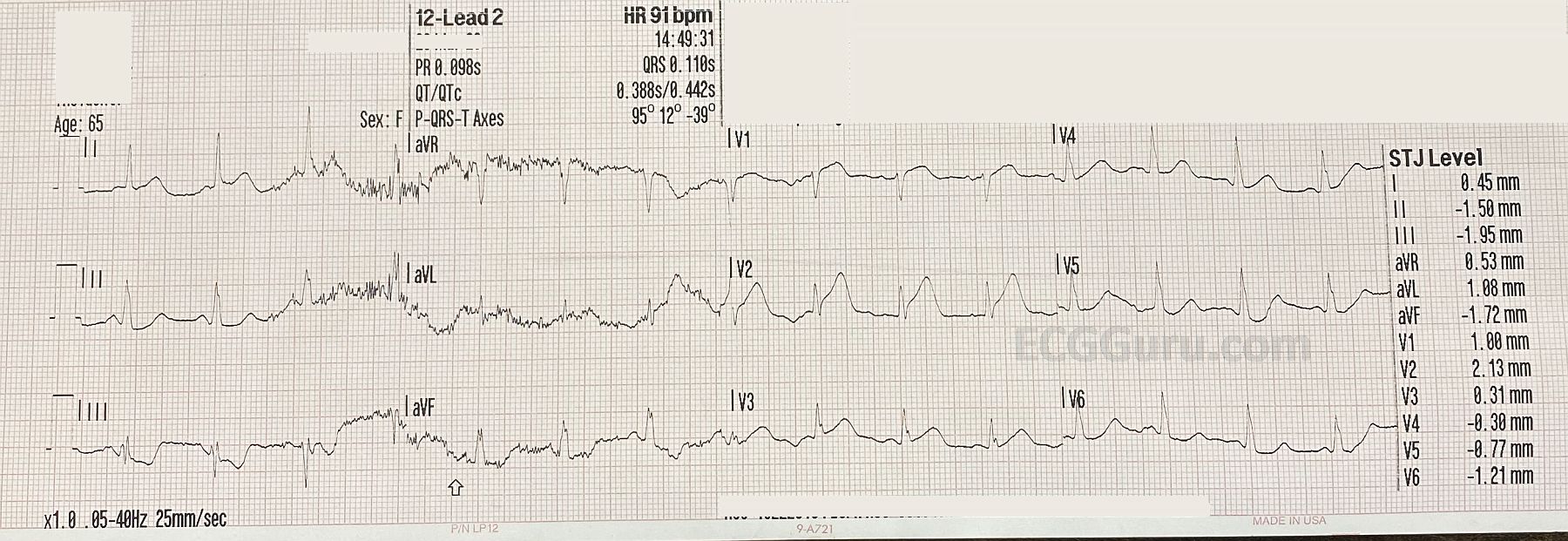
slight ST elevation in I and aVL with ST depression in II, III, and aVF. In chest pain, possible M.I., STD should be presumed to be reciprocal in nature. V1 has slight STE with a coved upward (frowning) appearance. V2 has more noticeable STE, with a tall, wide-based T wave. This is called a “hyperacute T wave”. We will have to evaluate V4 – V6 on ECG No. 2.
V4 Right has no ST elevation, and V8 and V9 have ST depression (reciprocal to the anterior leads). So far, we have all the signs of acute anterior wall M.I.