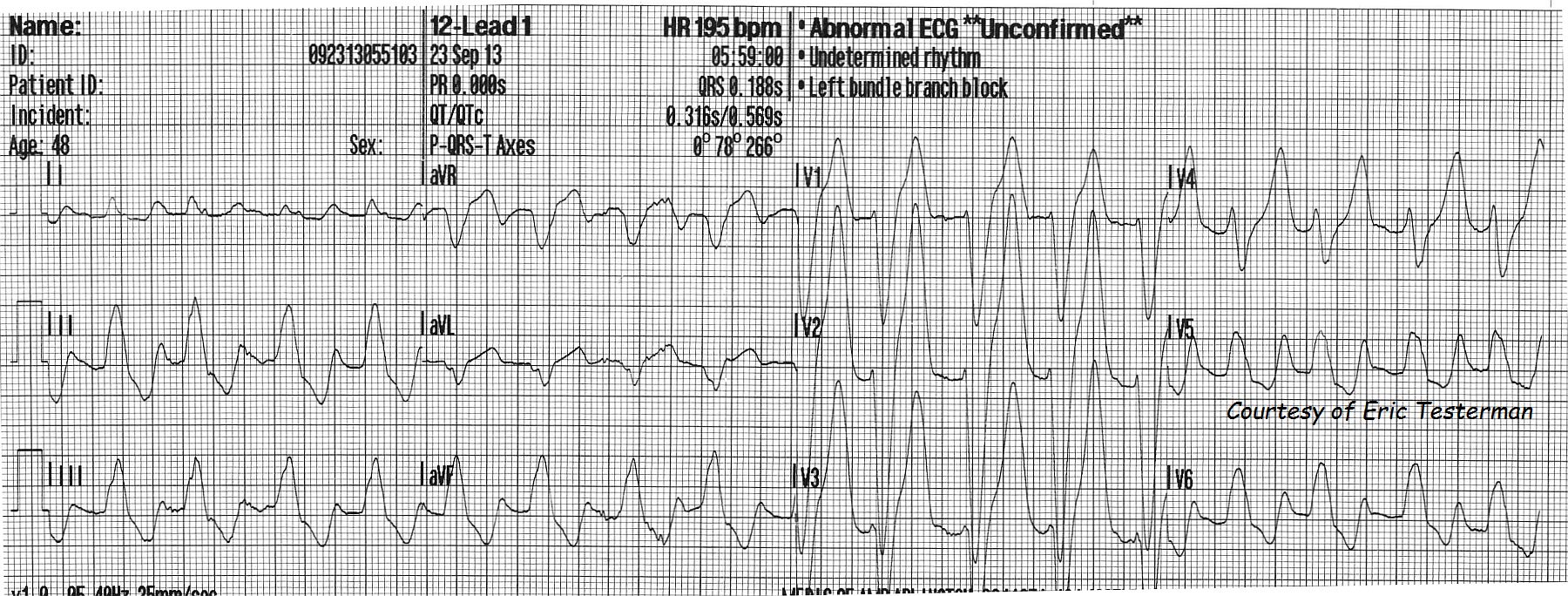
For your collection, we present another interesting set of ECGs from Paramedic Erik Testerman. They are from a 48 year old man who presented responsive only to painful stimuli, with deep, rapid (Kussmaul's) respirations. His blood glucose in the field read as "HIGH" - too high for the glucometer to register a number. He was treated with 3 large-bore IVs, 2 liters of NSS IV, O2. At the hospital, his blood glucose again registered as "HIGH" on the glucometer, arterial O2 was 90%, CO2 15 (low), pH 6.8 (acidotic), HCO3 -2 (depleted). His serum potassium was 7.0 ( greater than 5.5 is high ). We do not have the rest of his chemistry panel.
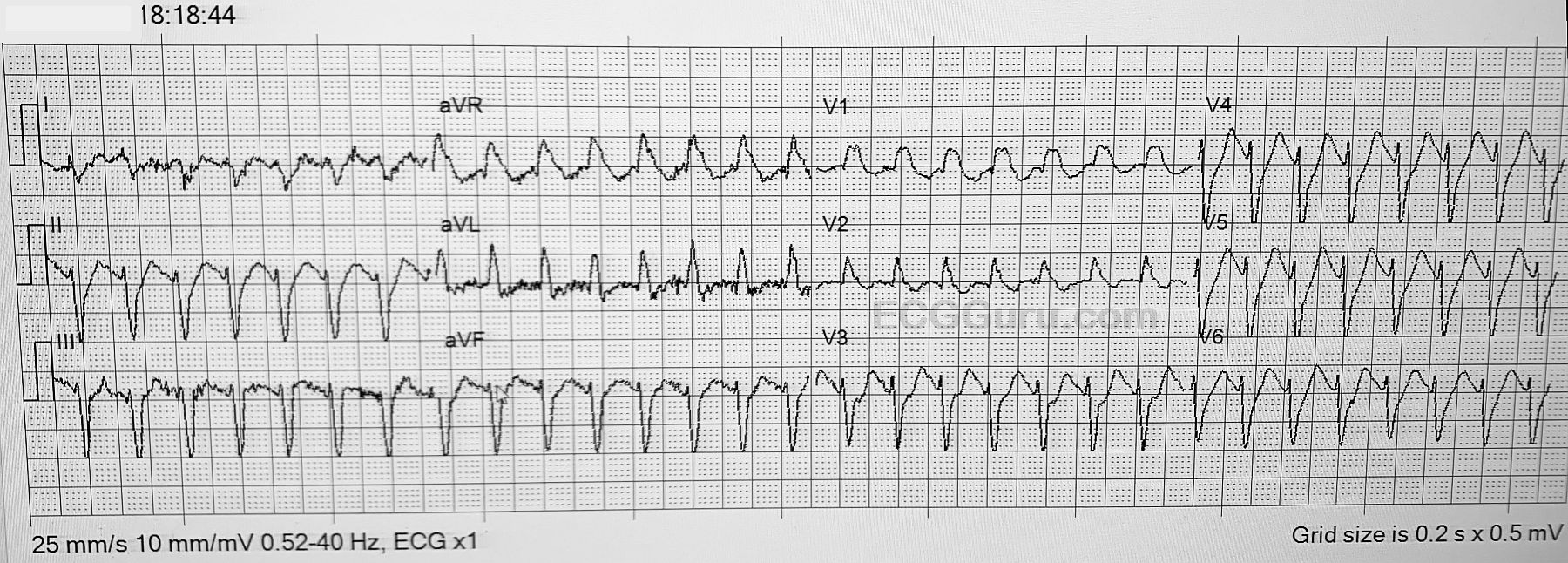
The first ECG, at 5:59 am, shows some signs of early hyperkalemia. One of these signs is wide QRS, at .188 sec (normal is less than .12). This ECG even meets the criteria for LBBB, as noted in the machine's interpretation, but the widening is more likely due to the high potassium. There is a right axis deviation. Left axis deviation is more likely in LBBB. LBBB pattern with right axis deviation can be a sign of biventricular enlargement, but, again, this may be an intraventricular conduction delay that is NOT LBBB. Another sign of hyperkalemia is that P waves are not evident. They can either be flattened until they disappear, or the PR interval can become so long the P wave is lost in the preceding T wave. The T waves are unusually tall and peaked in the chest leads - disproportionate to the wide QRS complexes. There are ST depressions in the inferior leads.
For a good, systematic approach to the ECG changes associated with hyperkalemia, we recommend Life In The Fast Lane, by Ed Burns.
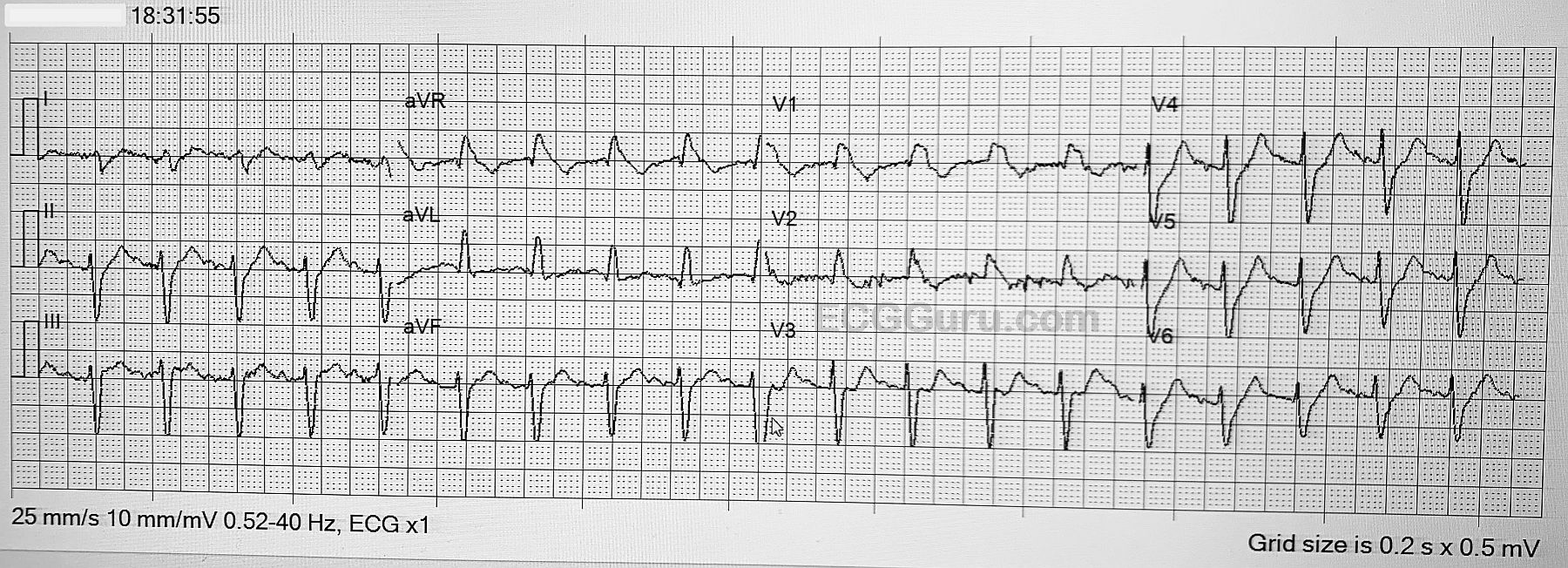
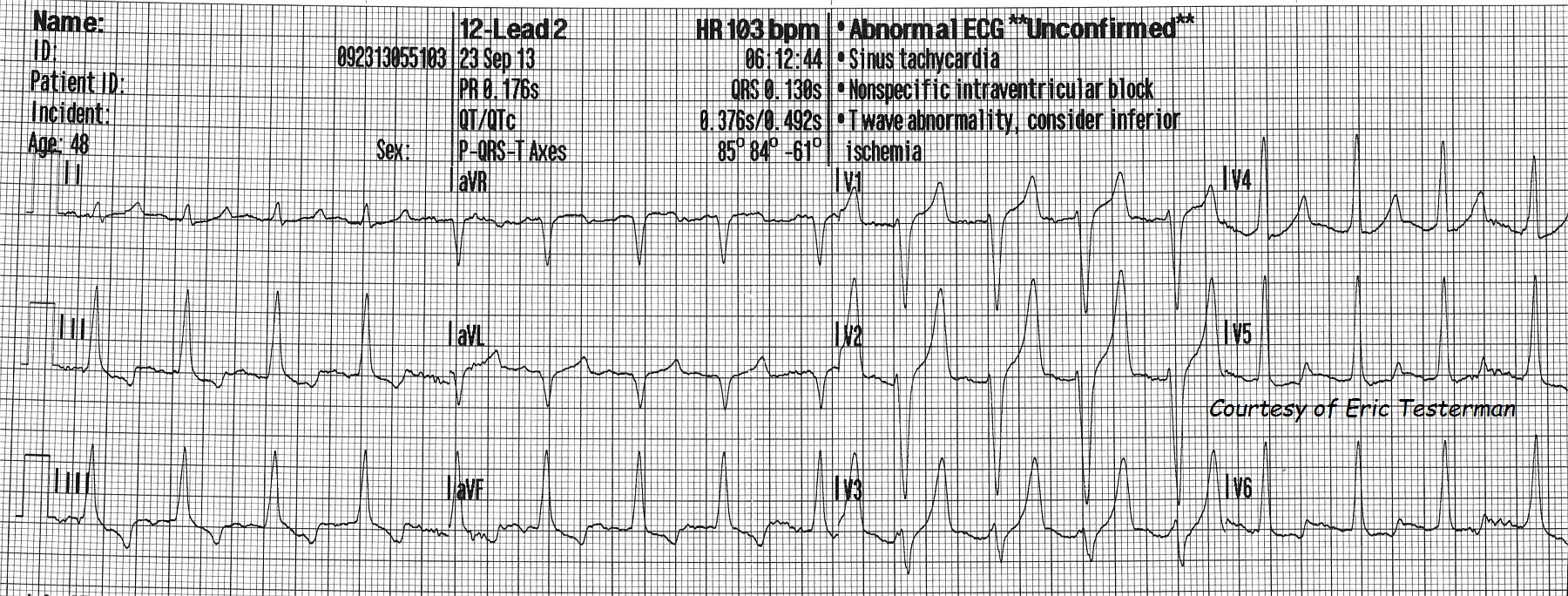
ECG number 2 was taken 13 minutes later, still in the pre-hospital phase. The QRS is now .13 seconds, and the tall, narrow, peaked T waves are very evident in Leads V1 through V3. There is T wave inversion and ST depression in the inferior leads. These are all possible signs of hyperkalemia, but also of other conditions. Unfortunately, hyperkalemia is a "mimic" of many conditions on the ECG. For a very interesting discussion of this topic, please go to Dr. Amal Mattu's ECG Discussion of the Week, October 14, 2013.