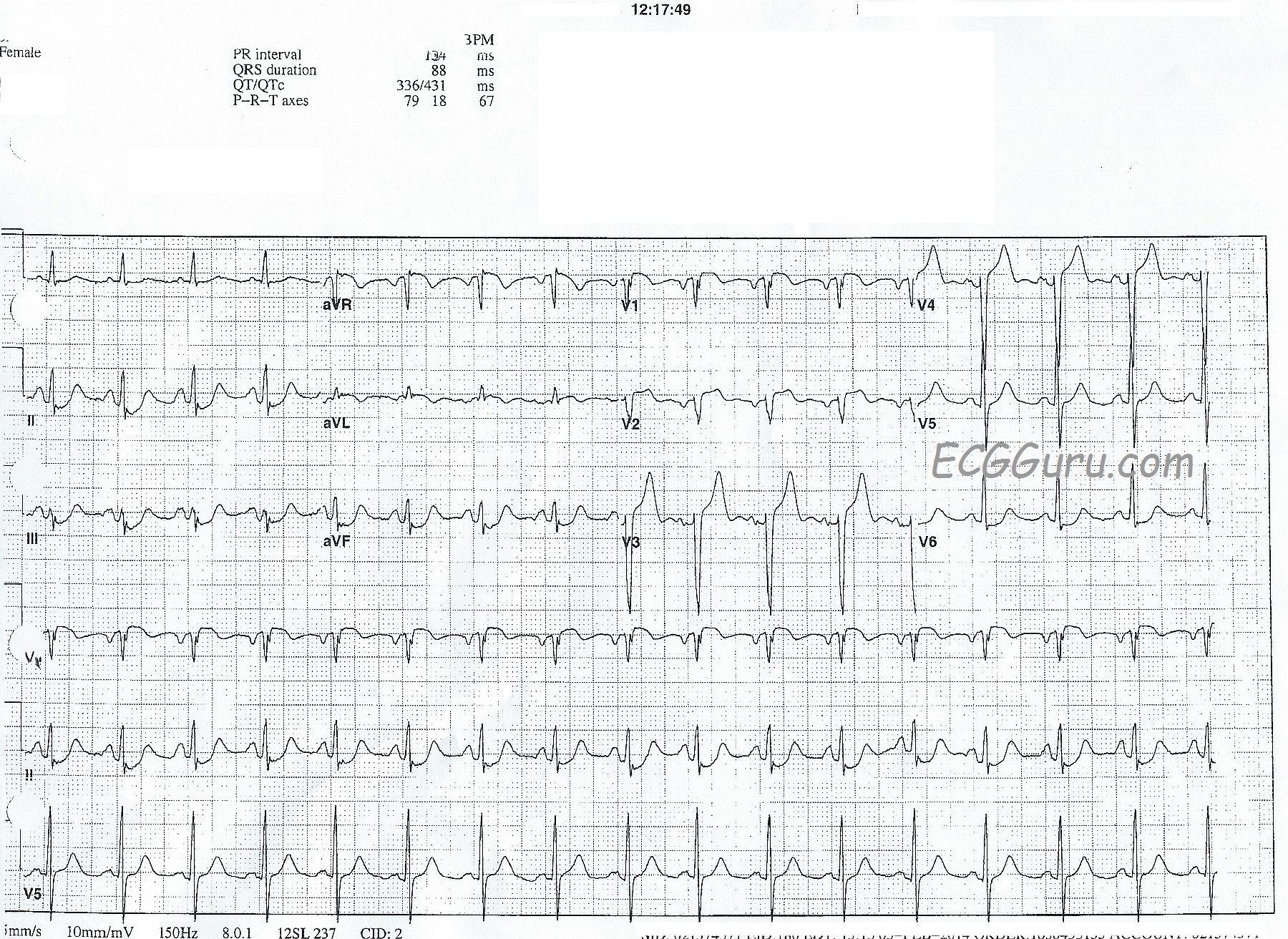
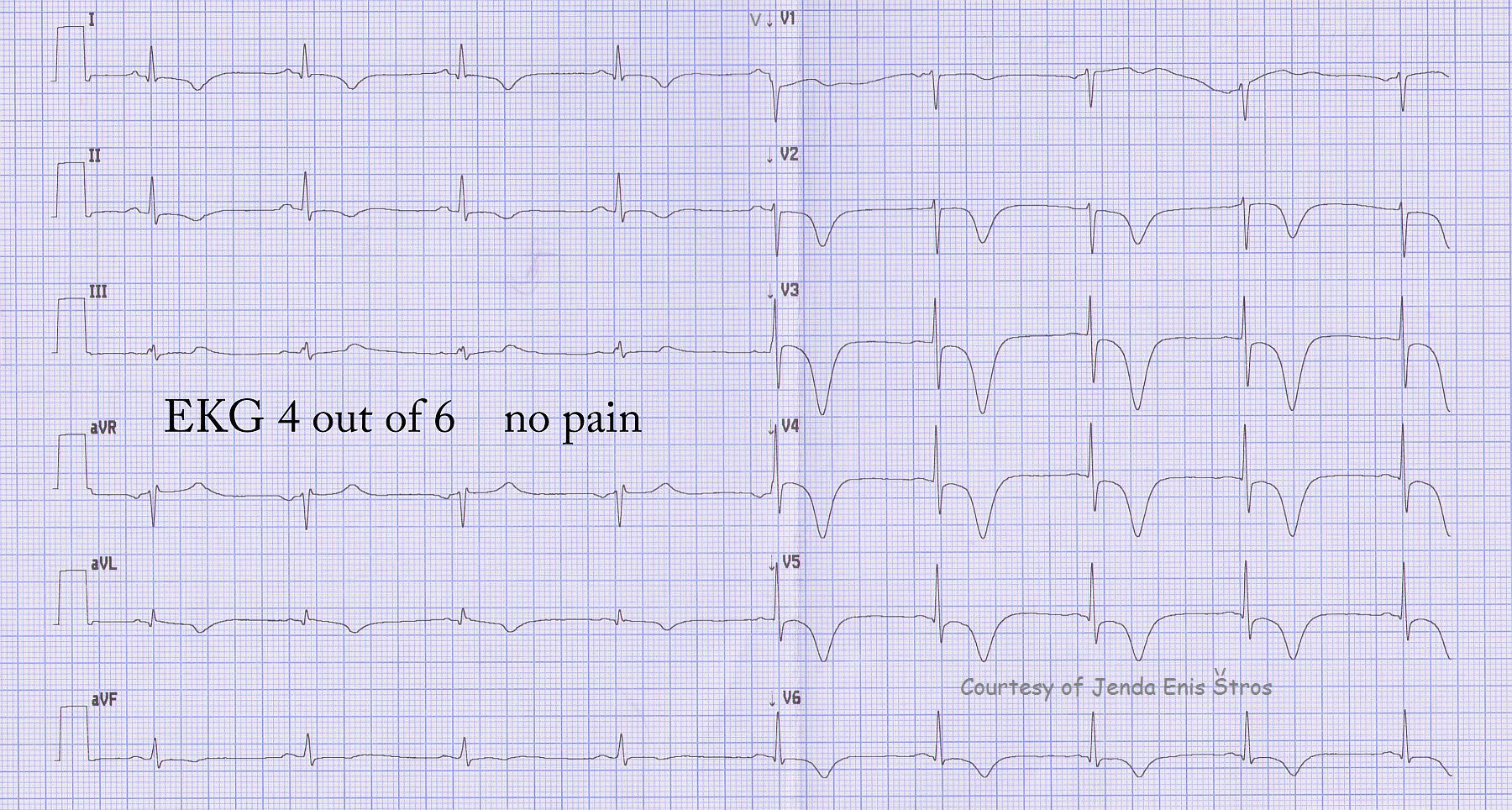
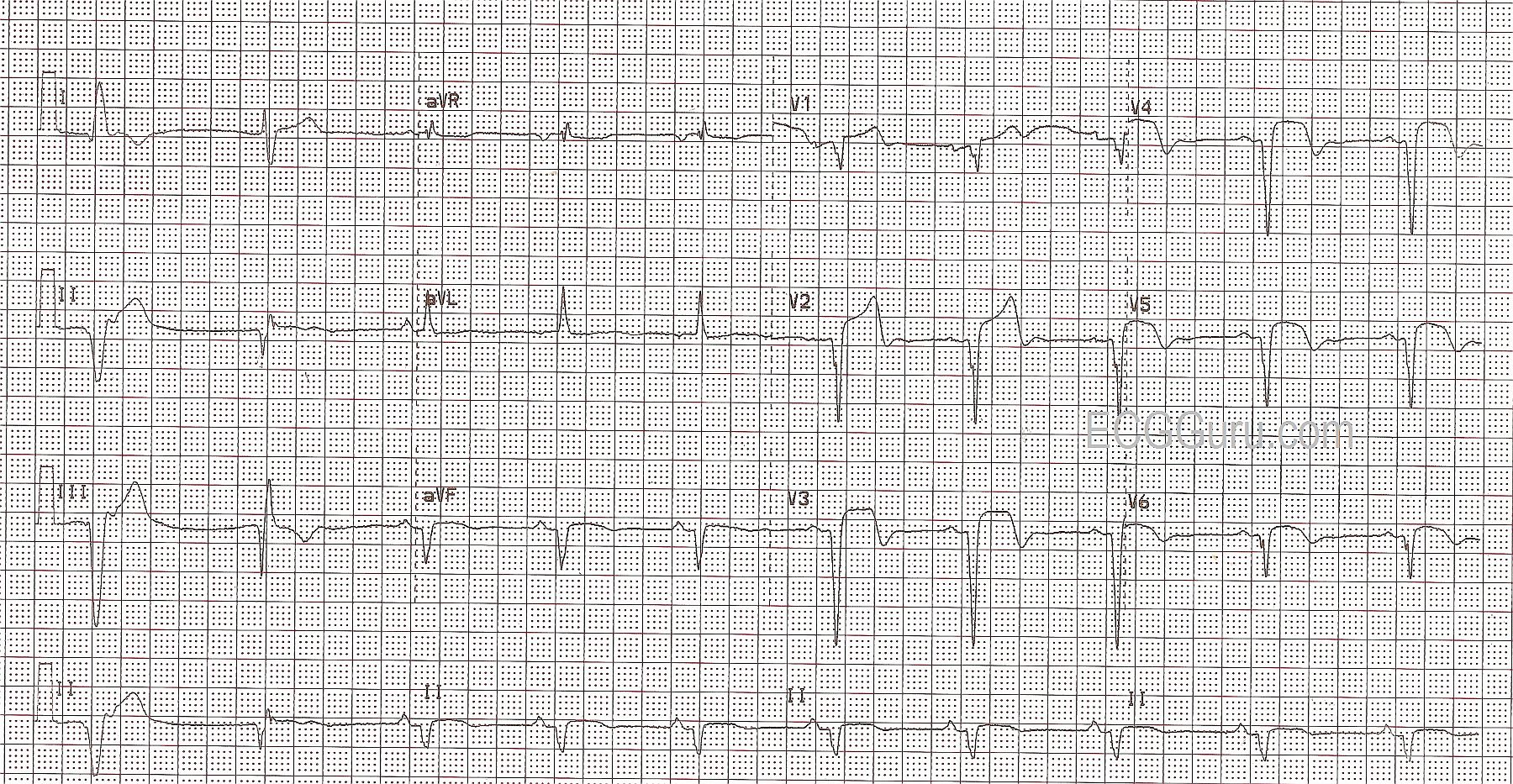
This ECG illustrates an acute anterior wall M.I. in a patient with a previous history of inferior wall M.I. The anterior wall M.I. can be seen in the classic signs in V1 through V6: ST elevations with coved upward shape (tombstones), T waves inverting beginning around V2 and continuing through V6, and pathological Q waves in V1 through V6.
The patient had a history of previous inferior wall M.I., unknown age. This is normally seen in Leads II, III, and aVF. The first two complexes on the strip are wide QRS complexes without associated P waves, presumably ventricular. It is impossible to know from this ECG whether the first complex is a PVC or escape beat, but the second appears to be escape. So, to evaluate the ST segments, T waves, and pathological Q waves in the inferior wall, all we have are aVF and the Lead II rhythm strip at the bottom. These show pathological Q waves (necrosis), and some slight elevation of ST, with coving or horizontal flattening. From this, we know there is damage in the inferior wall, but the age of the M.I. is undetermined.
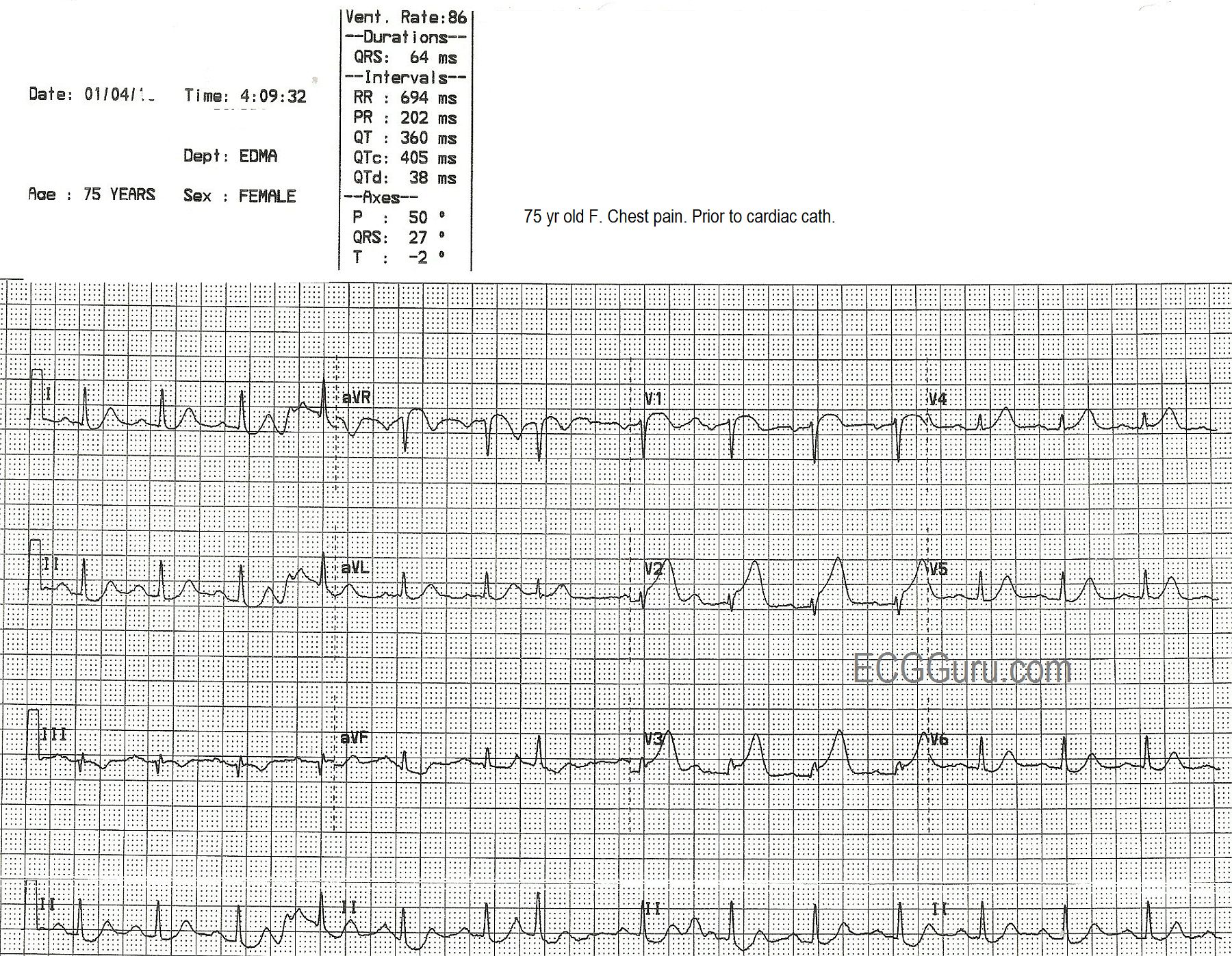
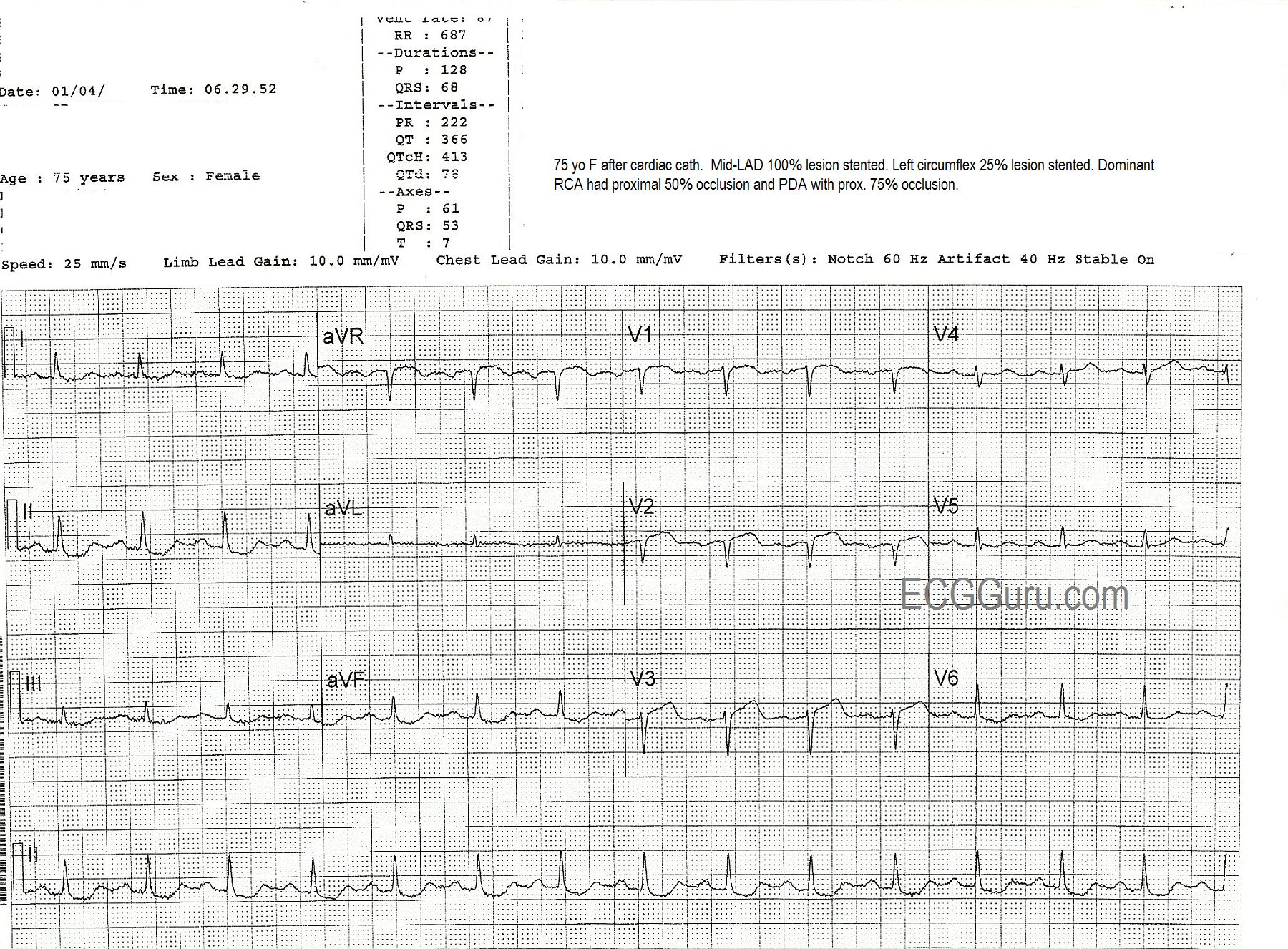
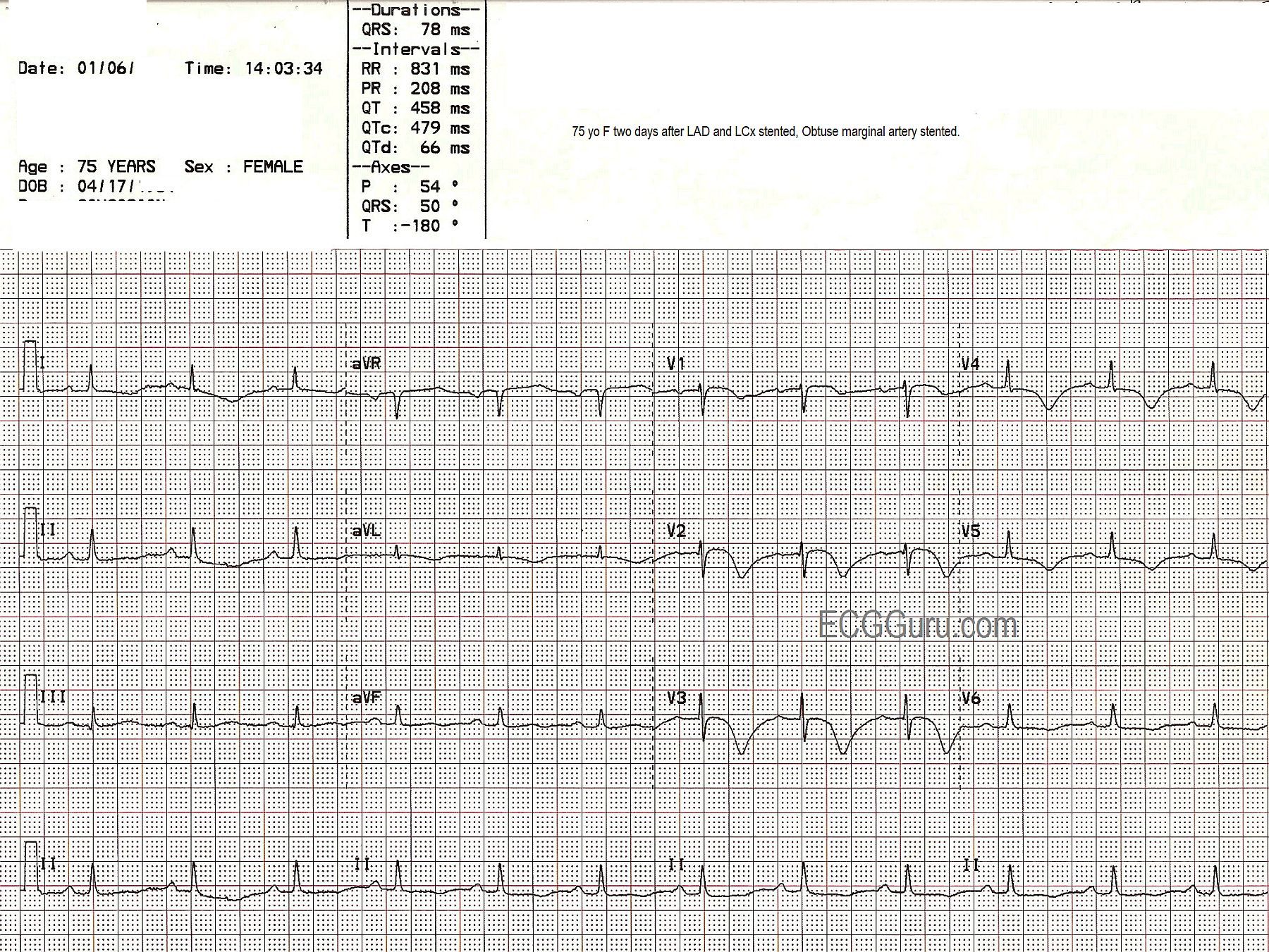
This patient went to the cath lab, and received angioplasty with stenting of the proximal left anterior descending branch of the left coronary artery.