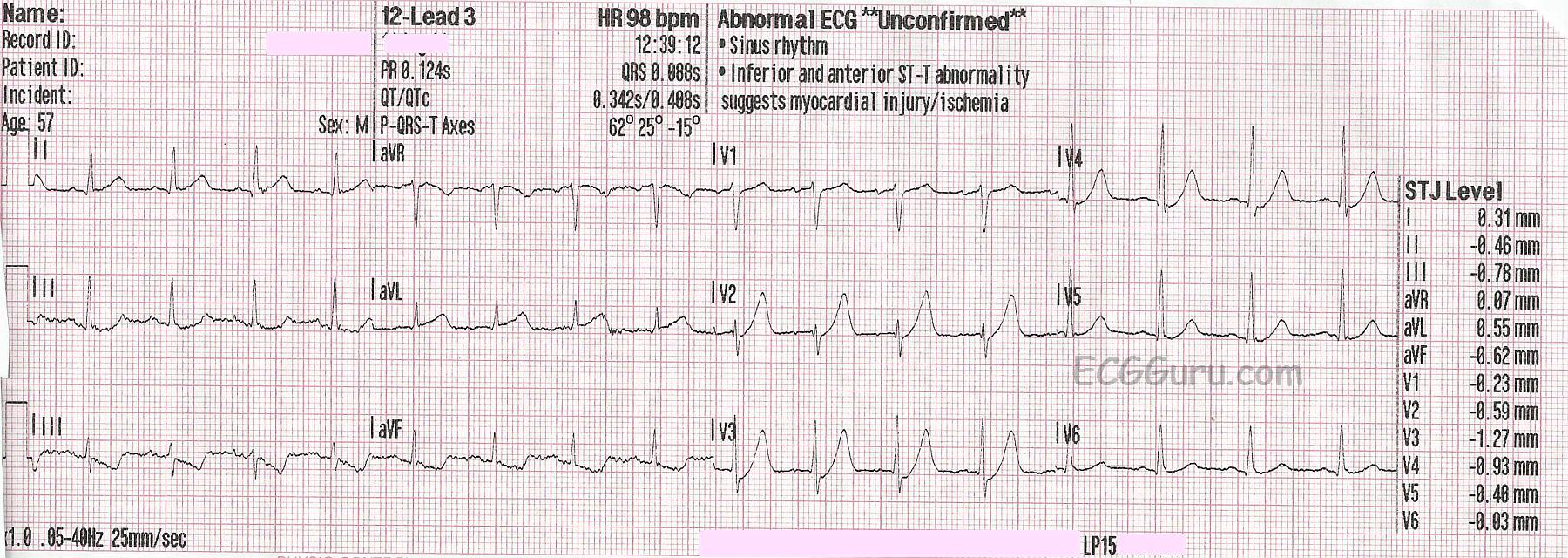
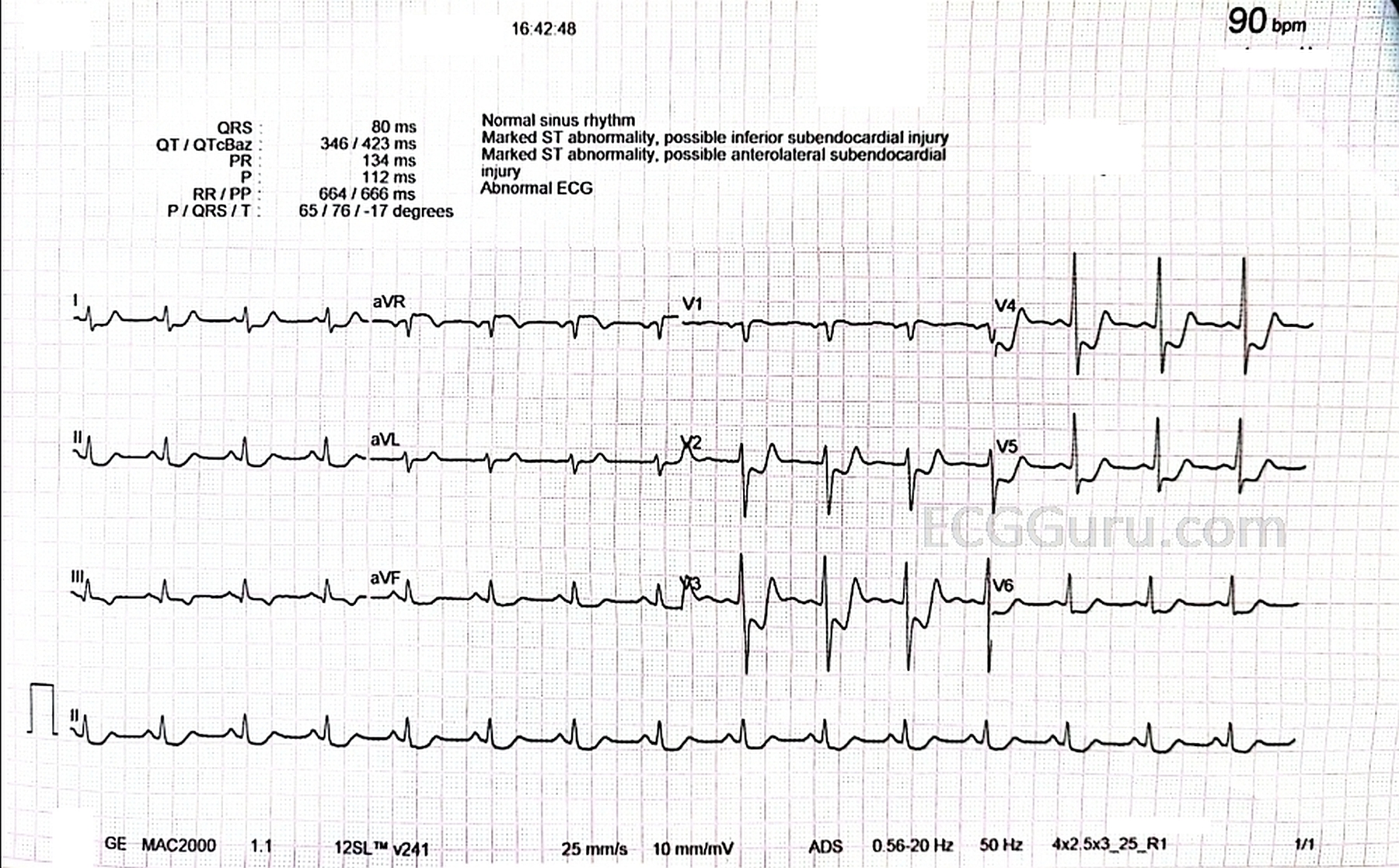
For many years we have misunderstood the concept of subendocardial ischemia as it manifests on the 12-lead ECG. Previously, if one saw ST depression in leads II, III, and aVF, it would be labelled "inferior subendocardial ischemia" and, if the patient were momentarily having little or no chest pain, the patiet would be sent home. The same thing happened with ST depression in leads V4 - V6; "anterolateral subendocardial ischemia," probably chronic and again, the patient may be sent home. And of course, ST depression in leads V1-V4: "anteroseptal subendocardial ischemia" and often the patient was sent home.
Then a number of years ago, some disturbing information began to surface in various medical journals around the globe. Sometimes ST depression that was limited to just leads II, III, and aVF, for example, did not reveal any actual subendocardial ischemia in the inferior wall of the left ventricle. In some cases, subendocardial ischemia was indeed present but very little involved the inferior wall and most of the ischemia was elsewhere; but... the only ST depression present was in the inferior leads. Some articles began mentioning the same findings regarding ST depression in other leads as well.
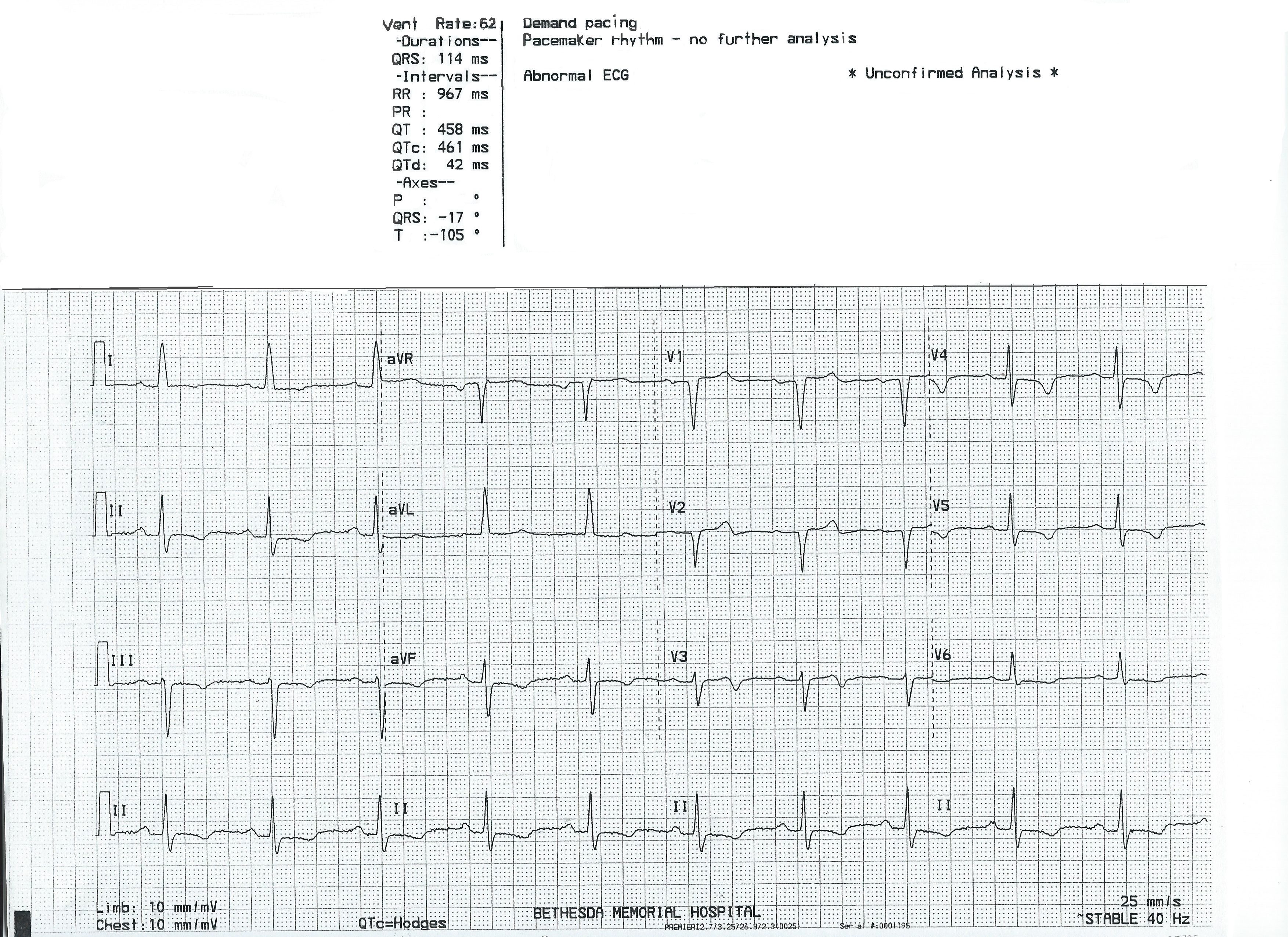
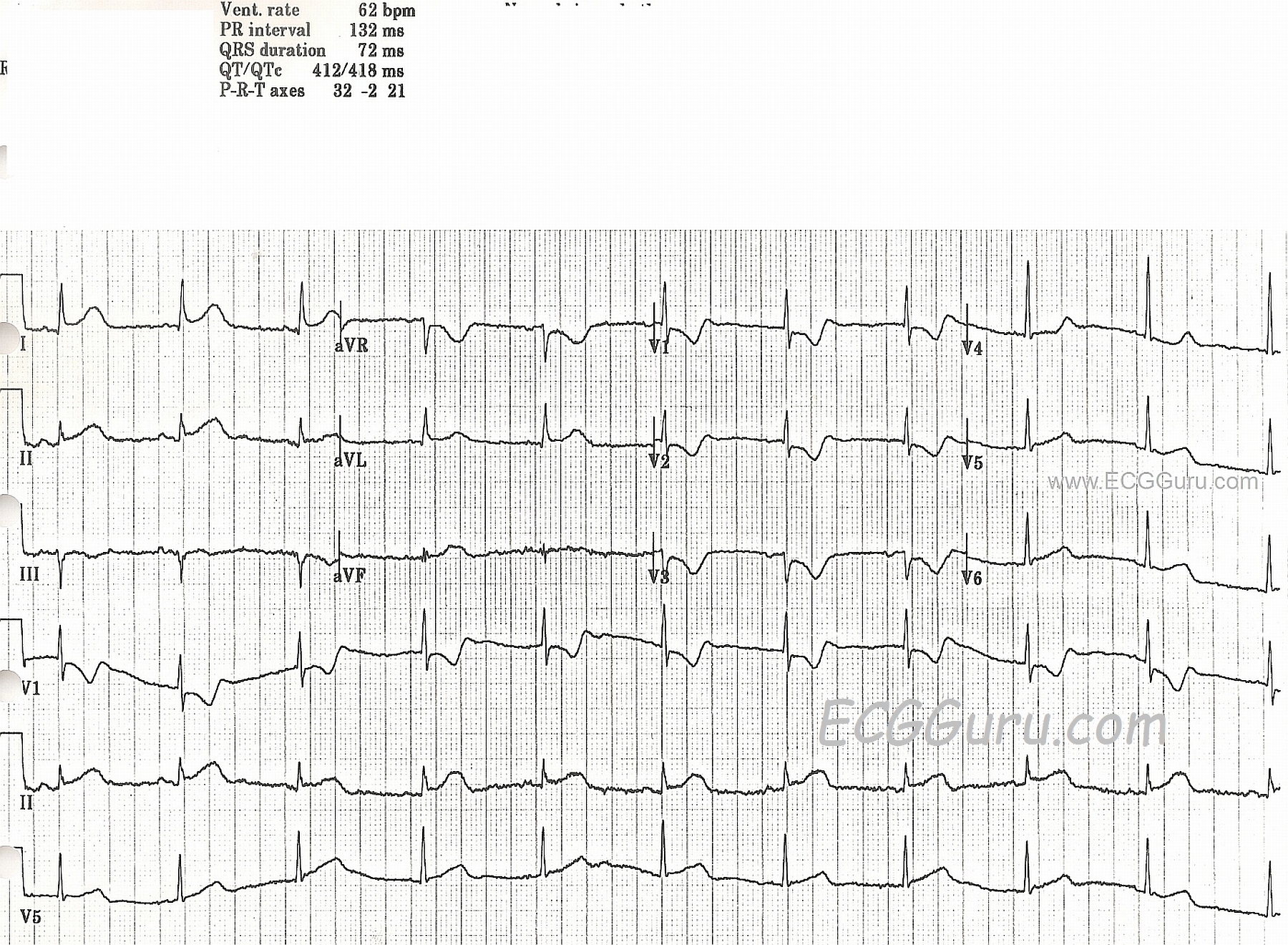
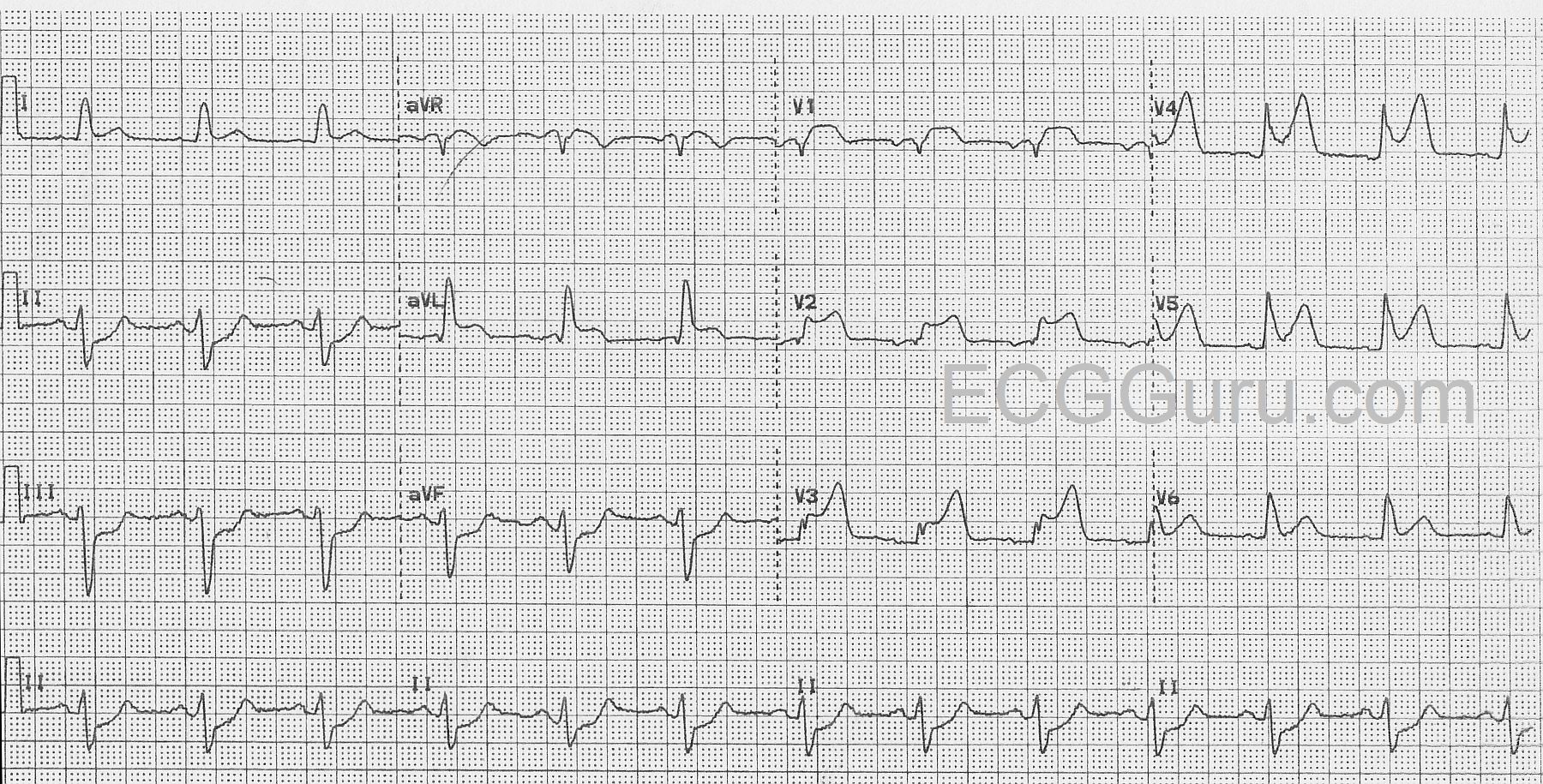
What we have learned is that when ST depression indicates subendocardial ischemia, IT DOES NOT LOCALIZE! Just because there is ST depression in leads II, III, and aVF does NOT necessarily mean that the ischemia is located in the inferior wall of the left ventricle. It MAY be there, or there may be SOME ischemia there but most of it elsewhere, or there may be NO ISCHEMIA AT ALL there.
Some people still have difficulty conceptualizing this, so I developed an allegory of subendocardial ischemia using the concept of a vacant house at night.

Imagine you have gone out for a walk one pleasant evening in your neighborhood. As you stroll down the street, you come upon a vacant house. You know it is vacant because the family that lived there moved out recently. However, you can see light coming from some of the windows of the house. You wonder what's going on, so you walk up to the house and look through a window into the living room. The room is illuminated but you don't actually see a light on there. You move around to another window and look into the dining room. Again, there is enough light for you to see everything in the room but you don't actually see any light fixture that is on. Finally, you move around to the window that looks into the kitchen. It's illuminated as well and you can see everything but, once again, the source of the light is not there. Is the light in a room that you cannot see or is it perhaps a closet light that has been left on somewhere in the house?
That - in essence - is subendocardial ischemia. Just because you see ischemia through the "windows" of leads II, III or aVF or the "windows" of leads V4 - V6 doesn't mean that the "source of the ischemia is in those "rooms."
Subendocardial ischemia manifested by ST depression does NOT localize reliably. So how should you report such ischemia? This is what I would say if I saw (for instance) ST depression in leads V4 - V6: "There is subendocardial ischemia present indicated by ST depression in leads V4 - V6." I would NOT call it "anterolateral ischemia."
Actually, this information has been available for a number of years. So, if you are reading textbooks, journal articles or posts on websites that still refer to "inferior ischemia", "high lateral ischemia", "anteriorlateral ischemia" etc., then you are reading information that is OUTDATED. If it was recently written, then you are reading information from someone who is NOT staying current with advances in electrocardiography.

 Dr. Jones has been on the teaching faculties of the University of Oklahoma and The University of Texas Medical Branch in Galveston. He is a published author who has also been featured in the New York Times and the Annals of Emergency Medicine for his work in the developing field of telemedicine. He is also a Fellow of the American College of Emergency Physicians and a Fellow of the American Academy of Emergency Medicine and, in addition, a member of the European Society of Emergency Medicine.
Dr. Jones has been on the teaching faculties of the University of Oklahoma and The University of Texas Medical Branch in Galveston. He is a published author who has also been featured in the New York Times and the Annals of Emergency Medicine for his work in the developing field of telemedicine. He is also a Fellow of the American College of Emergency Physicians and a Fellow of the American Academy of Emergency Medicine and, in addition, a member of the European Society of Emergency Medicine.