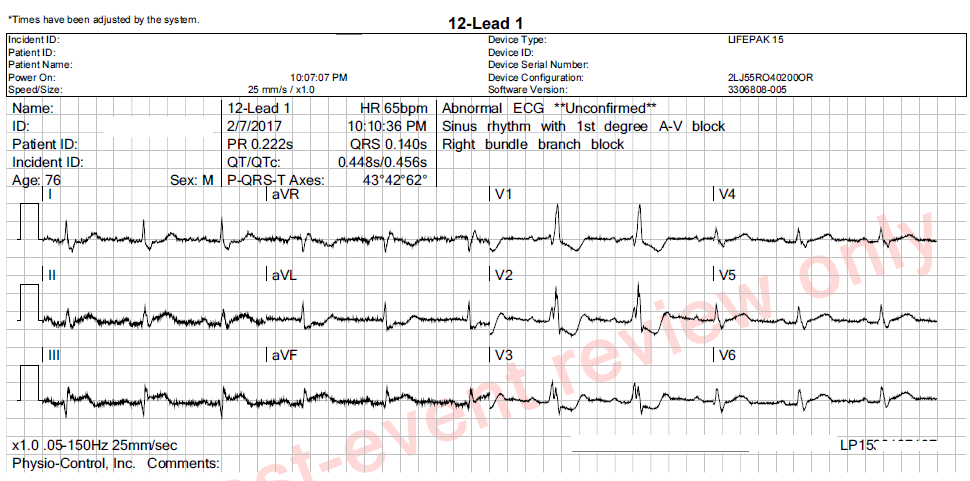
These ECGs were taken from a 76 year-old-man who was complaining of chest pressure for 20 minutes. He had a remote history of coronary artery bypass graft surgery.
This case has several good teaching points, including:
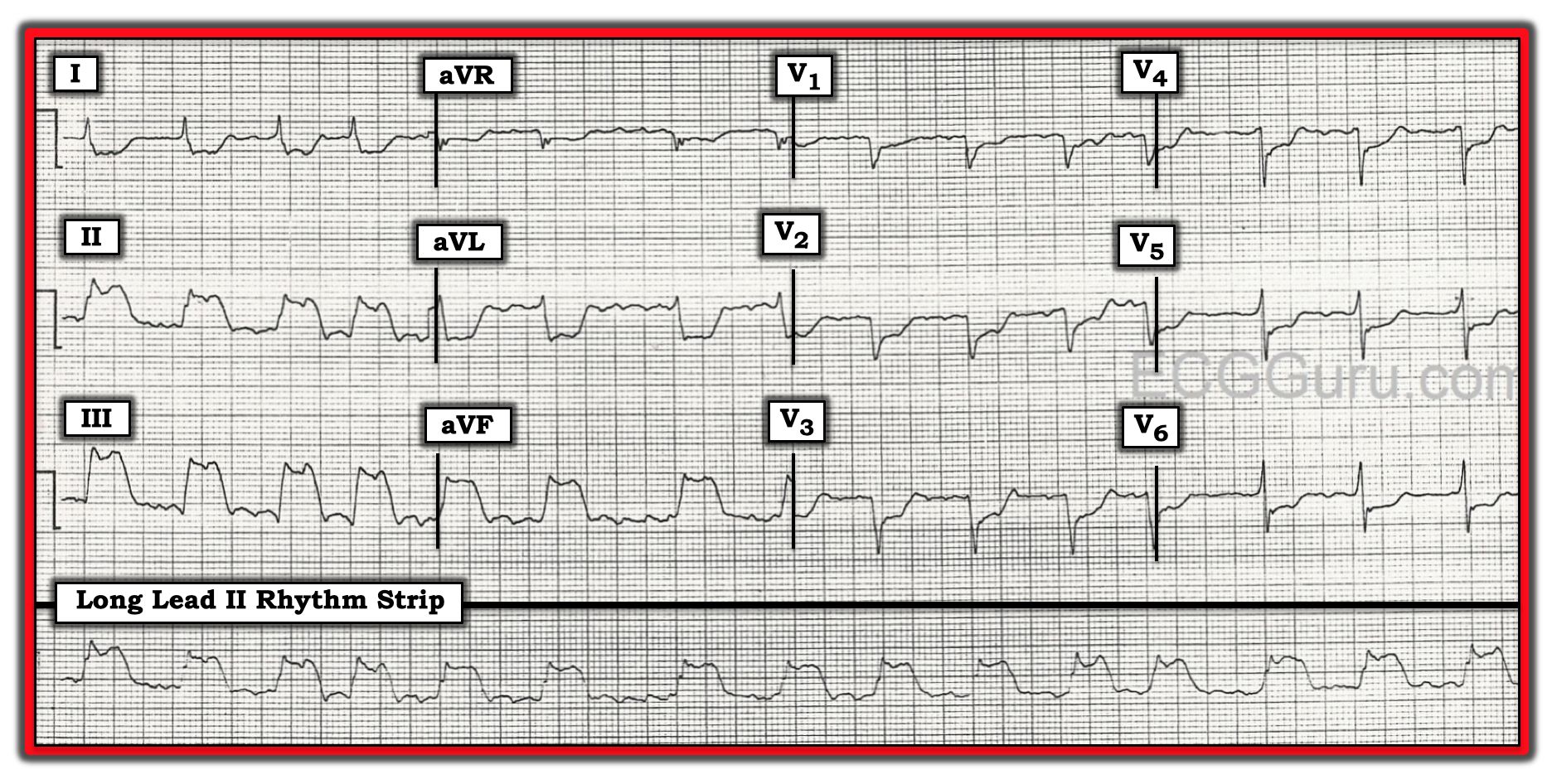
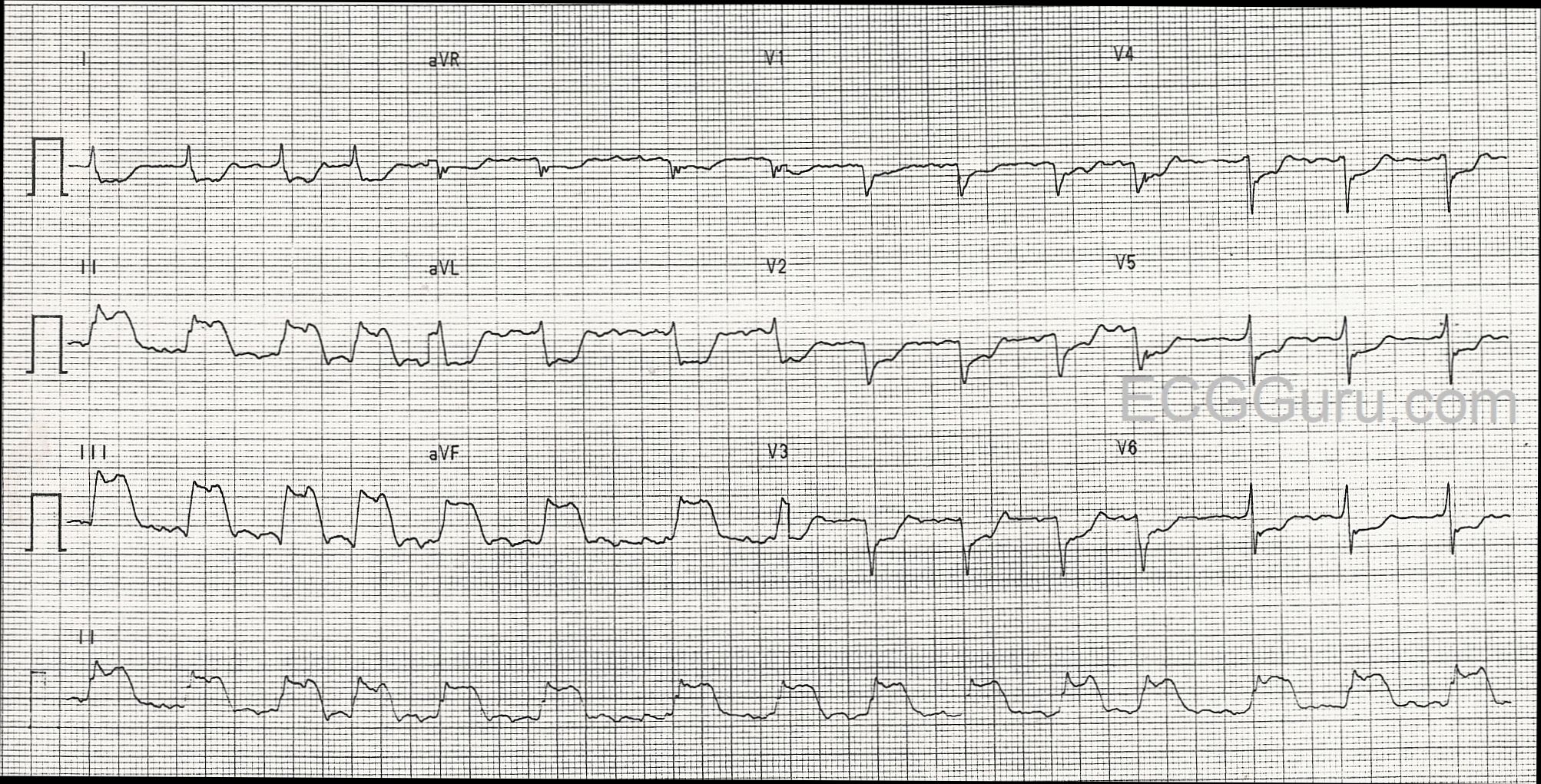
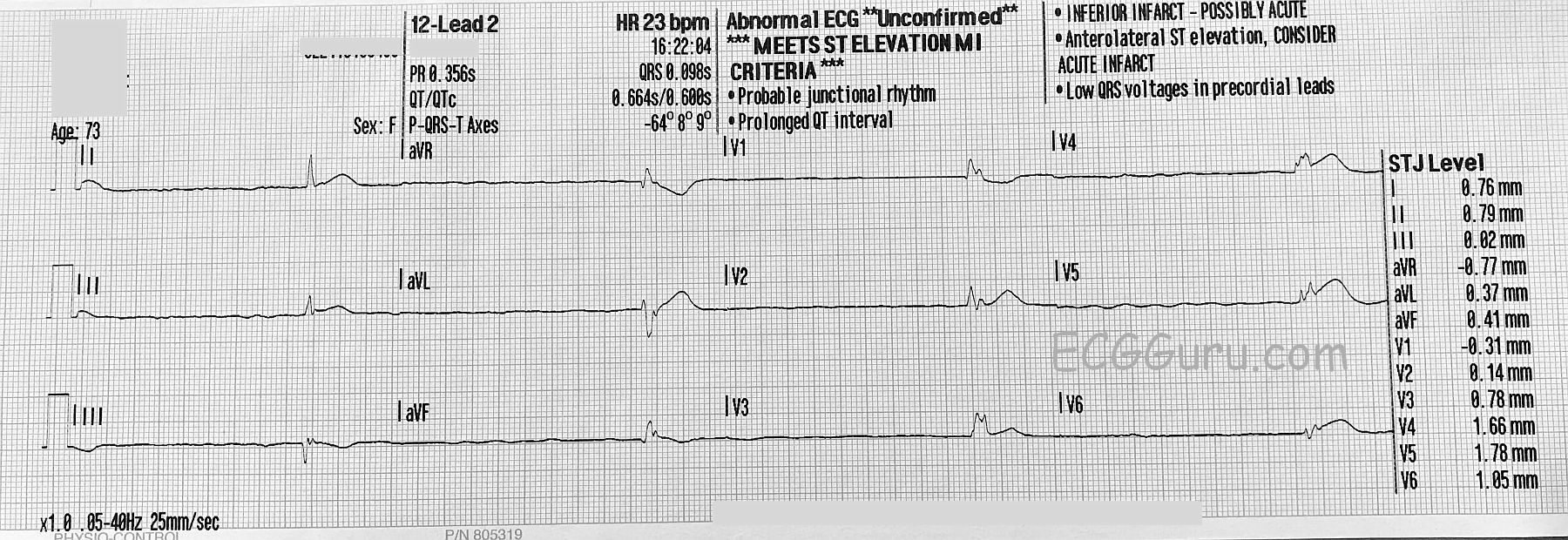
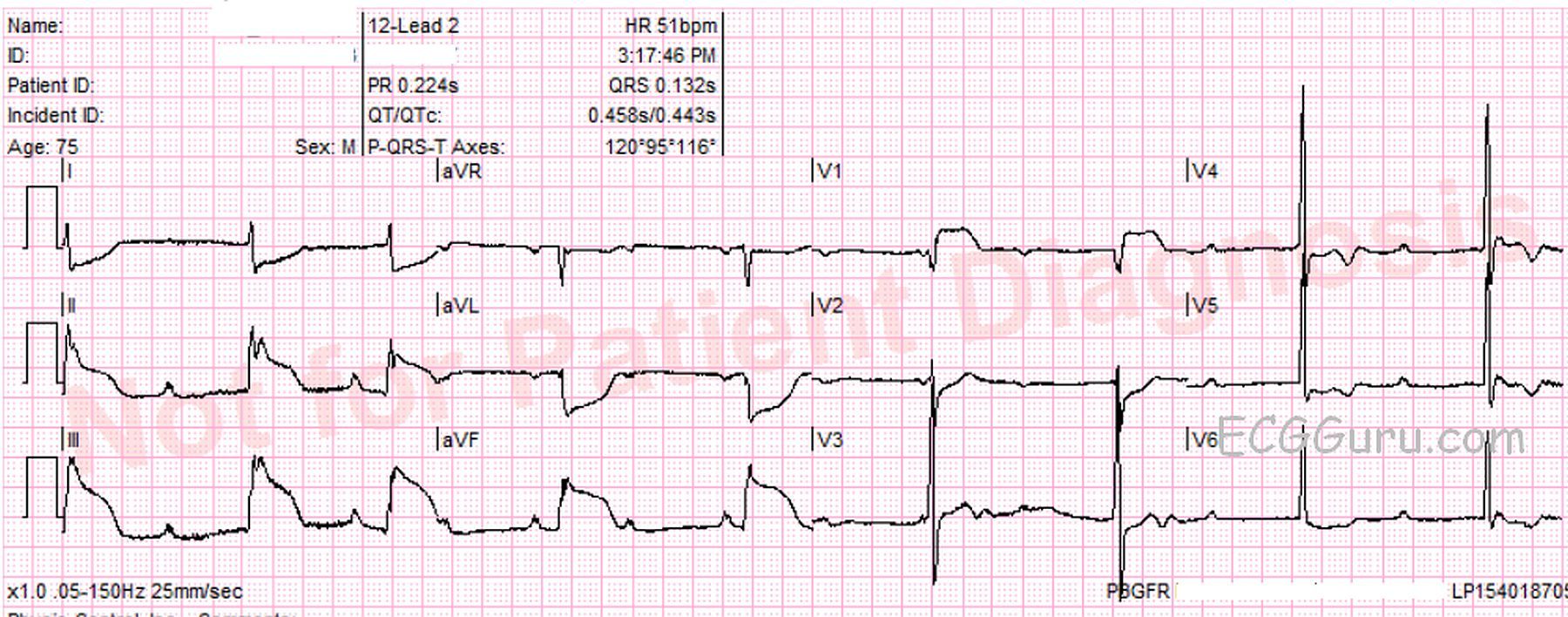
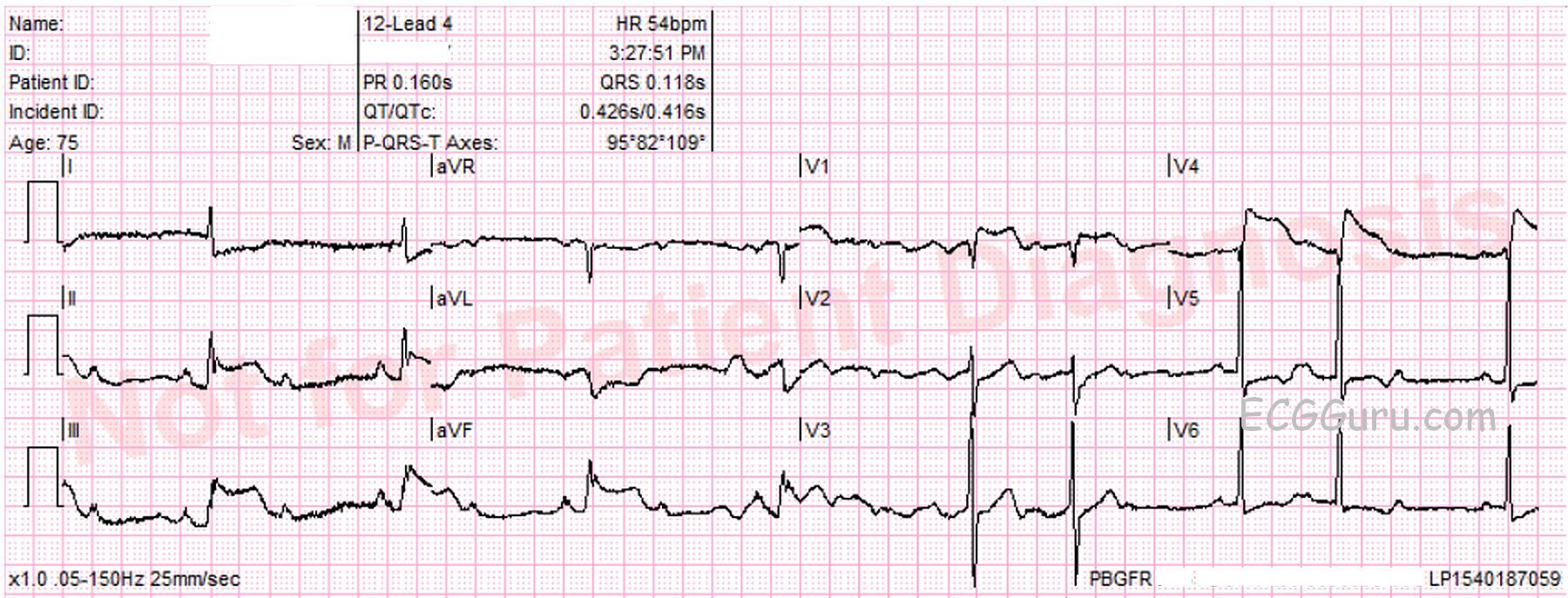
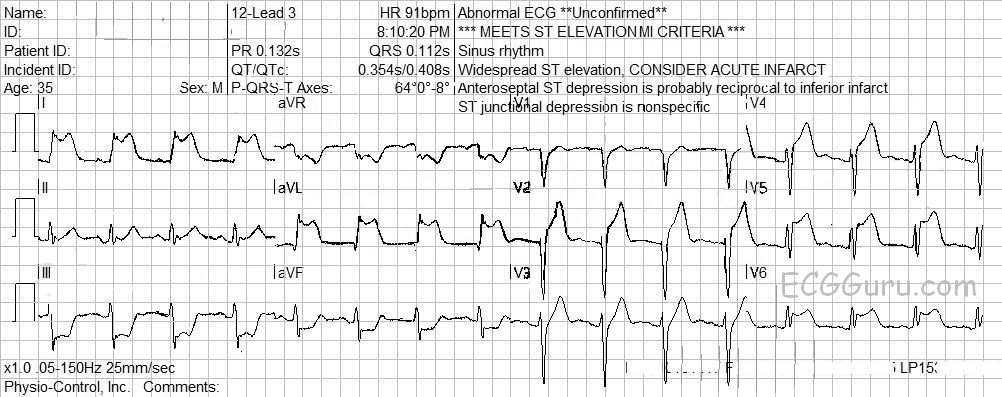
Significant artifact. The limb leads show artifact which is severe enough to hamper our assessment of the j point location. Every effort should be made to eliminate artifact. Some measures that might help are:
* clean and slightly "rough up" the skin where the electrode will be placed. A rough wash cloth or gauze pad will work.
* shave hair if necessary.
* avoid areas of movement if possible. Precordial electrodes must be placed in specific spots, but limb leads may be placed anywhere on the limb or on the trunk if it is impossible to avoid movement on the limbs.
* use fresh electrodes that have been protected from drying out.
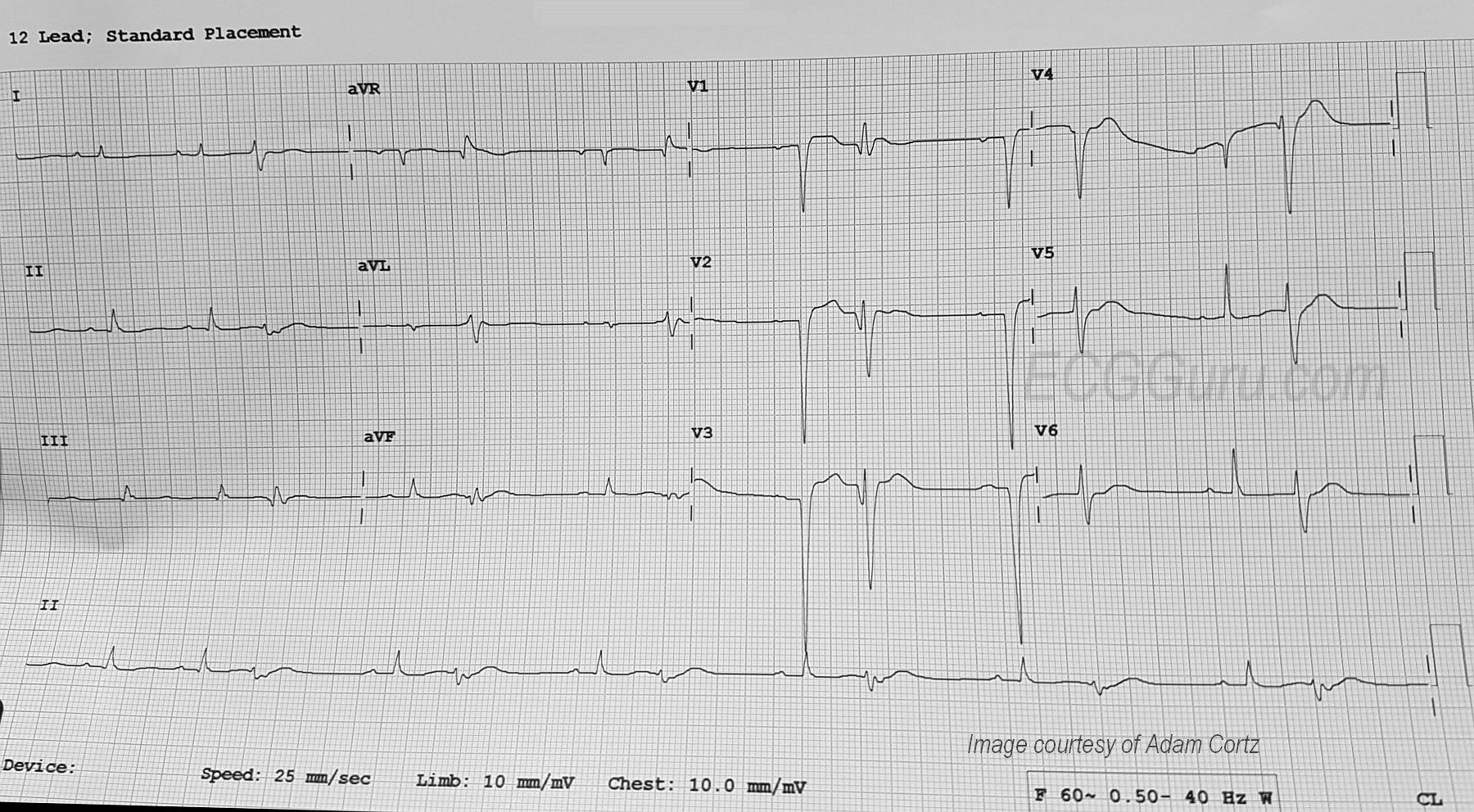
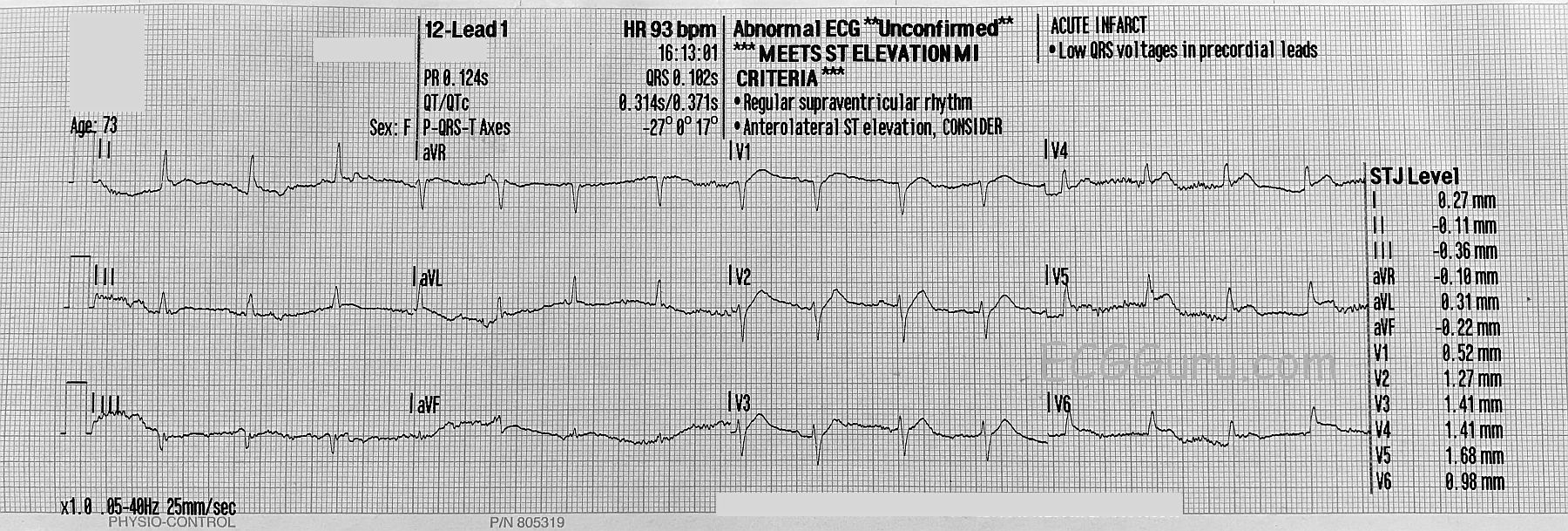
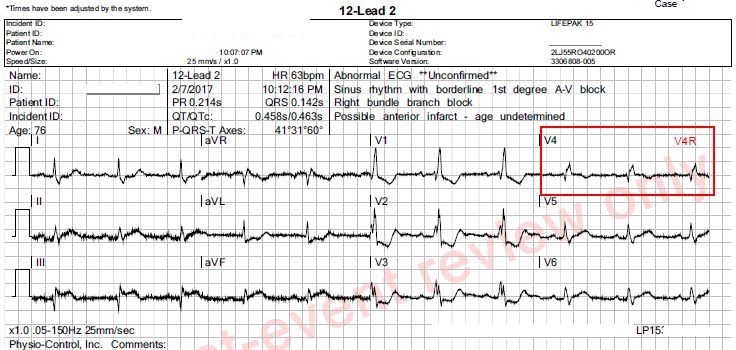
Subtle STEMI changes. This patient has an inferior wall M.I., which was confirmed as a complete occlusion of the right coronary artery in the cath lab. The ST elevation in Leads II, III, and aVF is subtle, and more difficult to measure because of the artifact. However, the SHAPE of the ST segments is a giveaway - they are very straight. A convex-upward shape is normal (see Lead I). Also, Lead aVL shows typical ST DEPRESSION, as a reciprocal view of the STE in Lead III. More ST depressions can be seen in Leads V1 through V3, and they end abruptly there. These localized ST depressions represent a reciprocal view of the posterior (also called lateral) wall, and represent an "extension" of the inferior wall M.I. up the back of the heart. A V4 Right lead was obtained and shows no measurable ST elevation, but the shape is straight to slightly "frowning", indicating that the right ventricle may soon have STE. Repeat ECGs should be obtained to watch for more definite ST elevations.