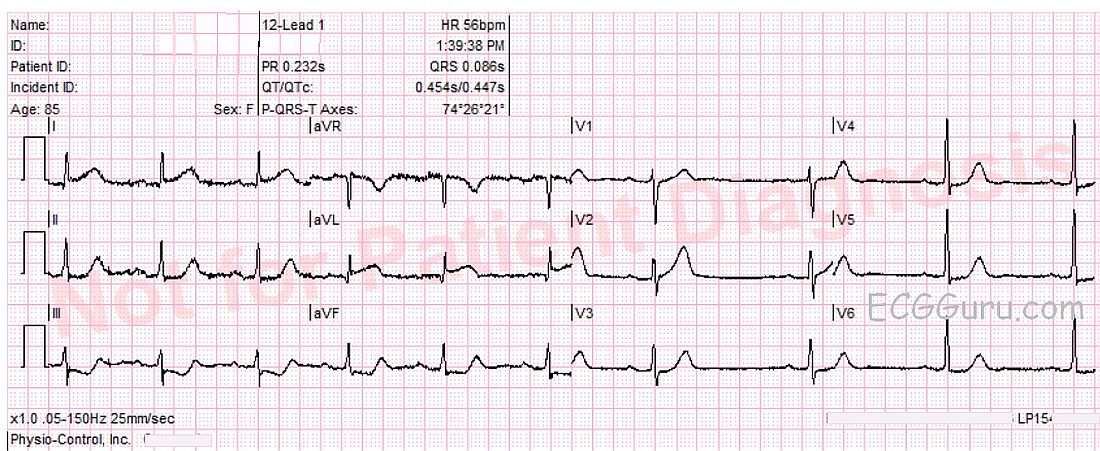
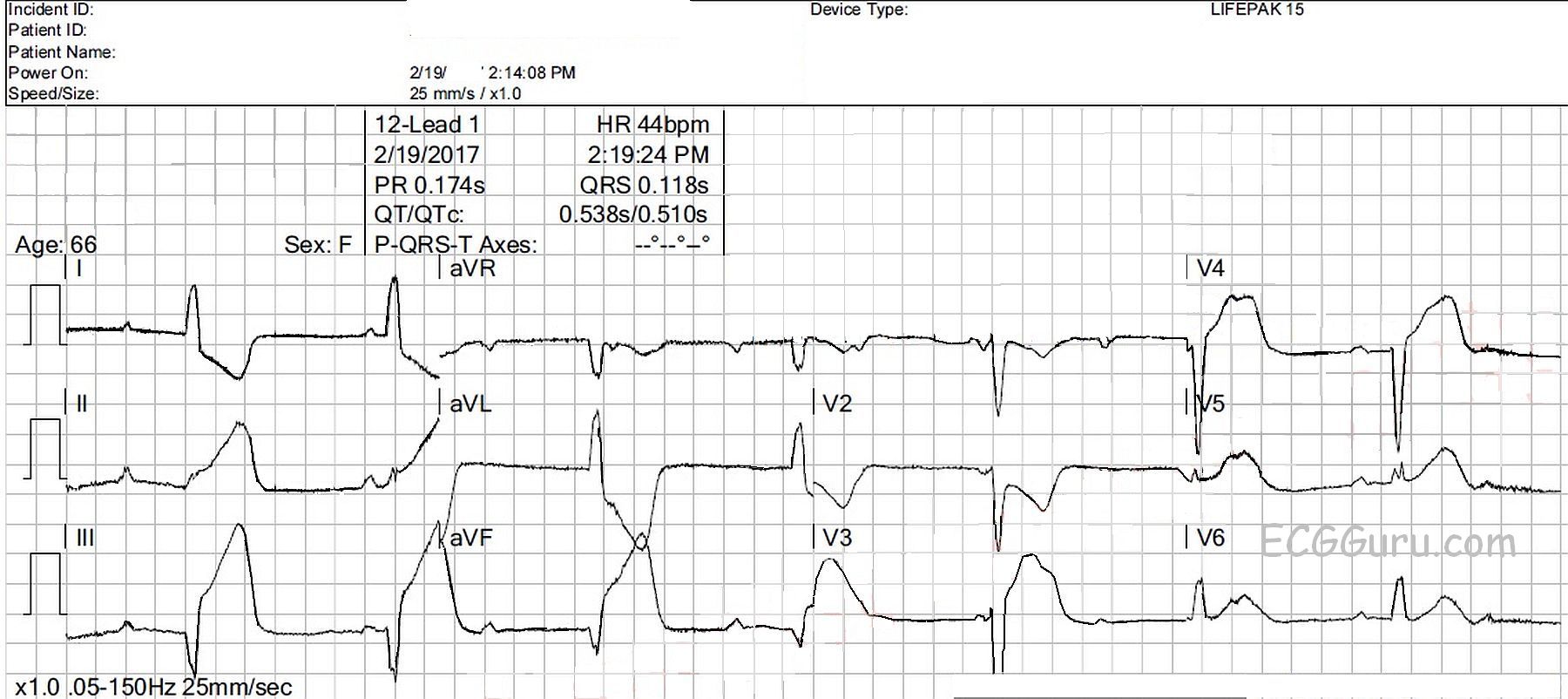
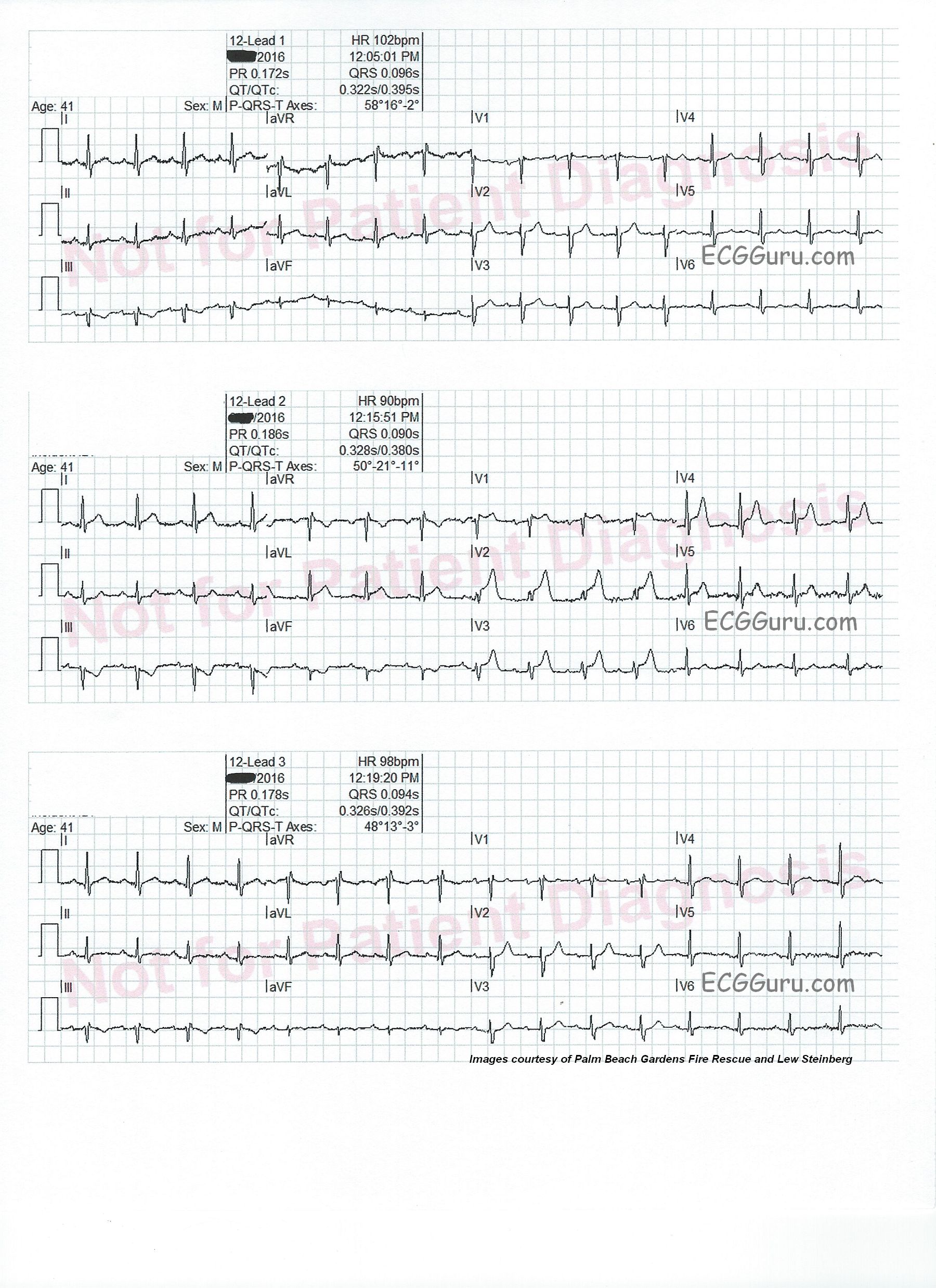
Intermittent chest pain. This series of three ECG were taken from a 41-year-old man with a two-week history of intermittent chest pain. At the time of the first ECG, 12:05 pm, he was pain-free. We see a sinus tachycardia at 102 bpm, and has just come under the care of paramedics. There is a very subtle ST sagging and T wave inversion in Lead III, and no other ST changes. He had an uneventful trip to the hospital.
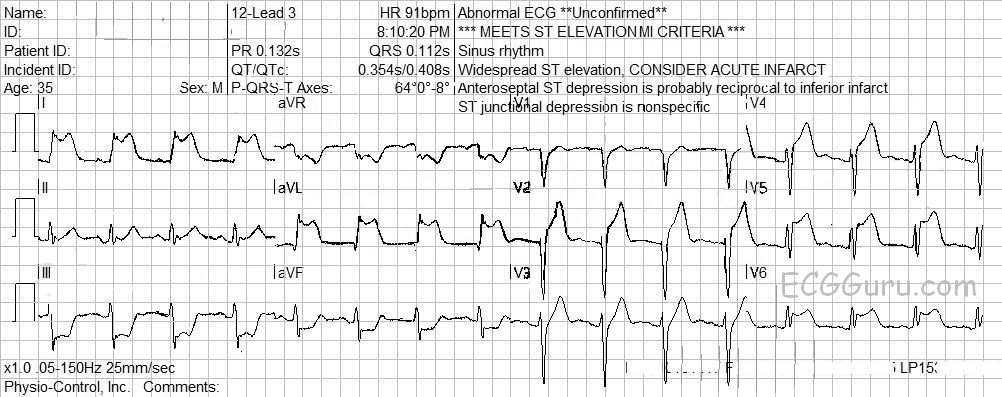
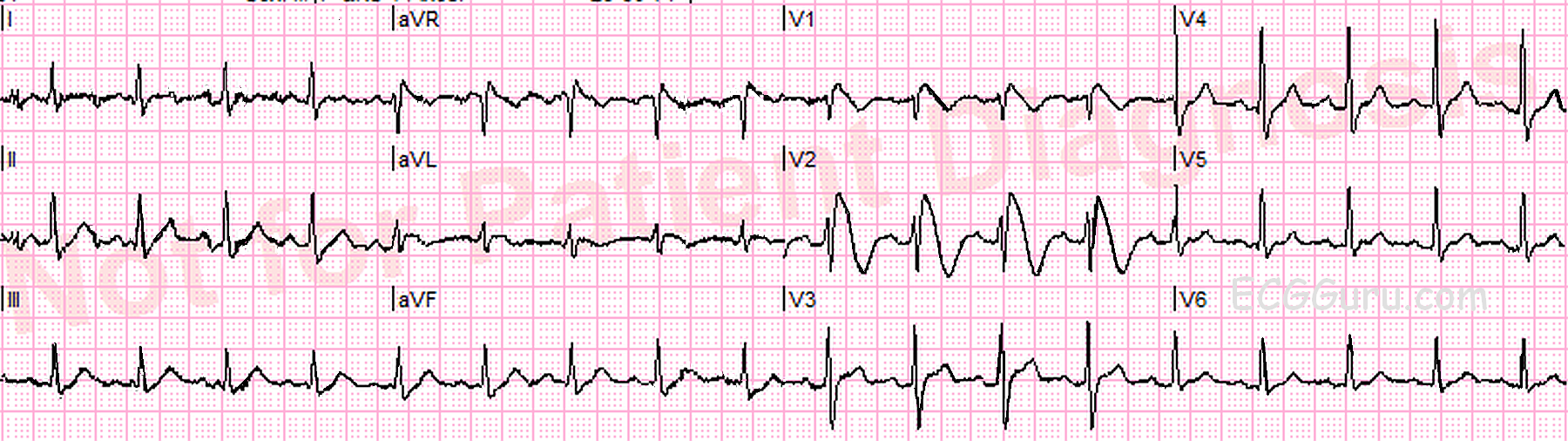
On arrival at the Emergency Department, just before he was unloaded from the ambulance (12:15), he experienced chest pain. An ECG was obtained, which shows ST elevation in V1 through V4, as well as in Leads I and avL. There are reciprocal ST depressions in Leads III and aVF.
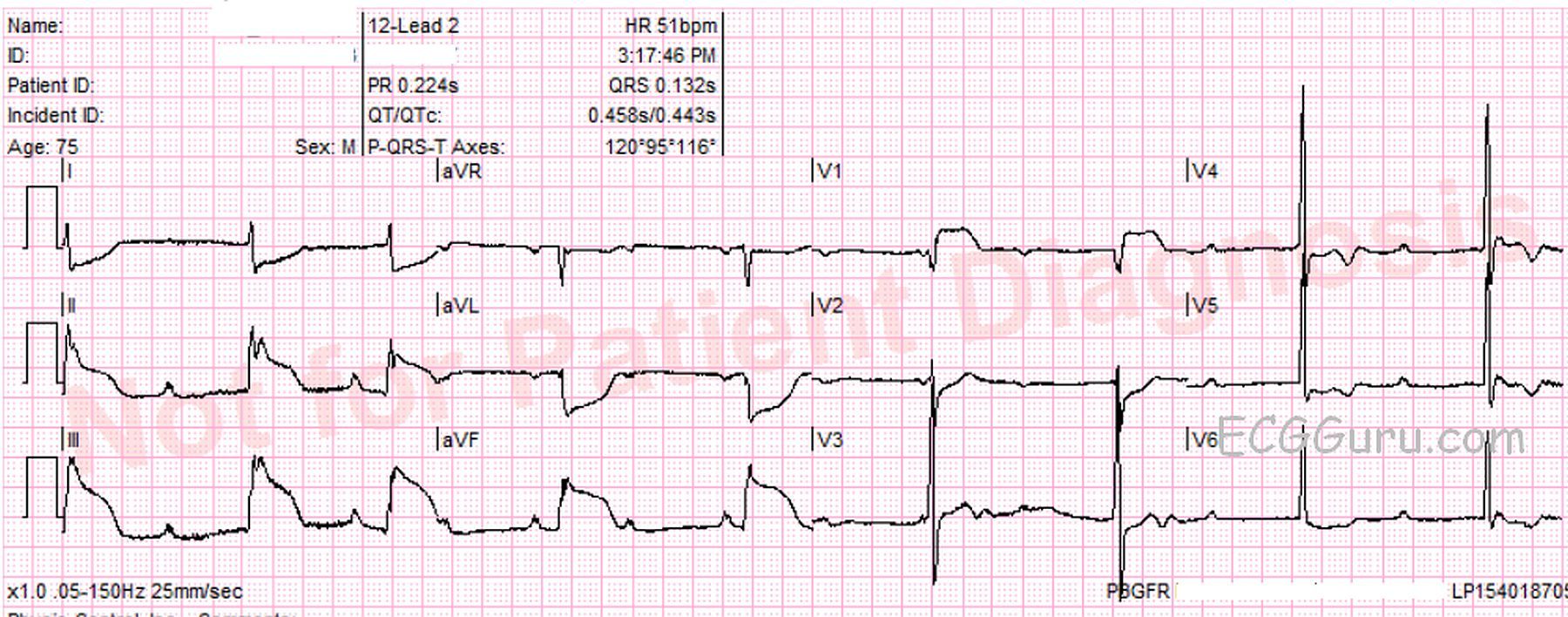
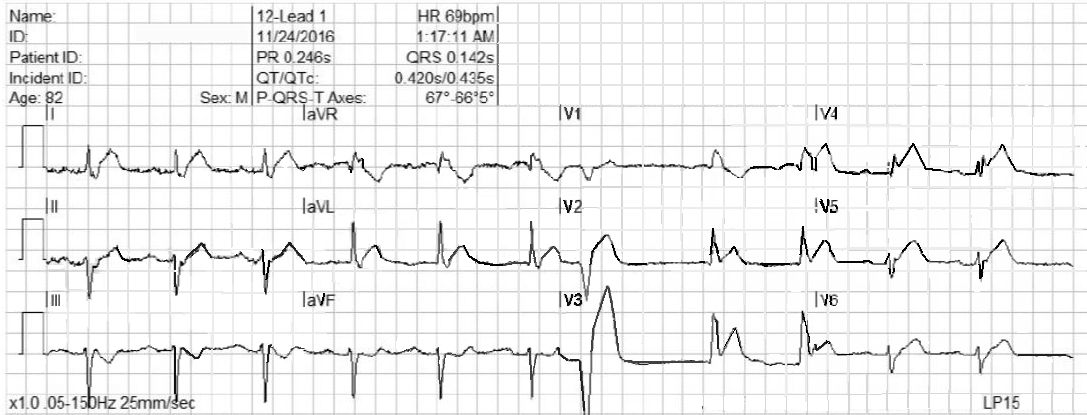
The patient was taken into the ED, where his symptoms abated, and a third ECG was obtained (12:19). The third ECG looks very much like the first one. V5 and V6 have T waves that appear flat, or even inverted, but there is some baseline artifact making it hard to see them.
Diagnosis confirmed Based on the patient’s presentation, and the second ECG, he was taken immediately to the cath lab. A 100% occluding lesion with a clot was discovered in the mid LAD. The clot was removed with suction, and the lesion stented. A 40% narrowing was discovered in the RCA.
Repeat ECGs whenever possible This series of ECGs offers a compelling argument for performing repeat ECGs. This can be especially important when symptoms are waxing and waning. Sometimes, a clot can completely occlude an artery, then “float” to another position, allowing blood flow to resume. Sometimes, the artery constricts around the lesion, causing occlusion, then relaxes. Had the rescue crew not repeated the ECG at 12:19, there may have been a delay in this young patient receiving interventional care.