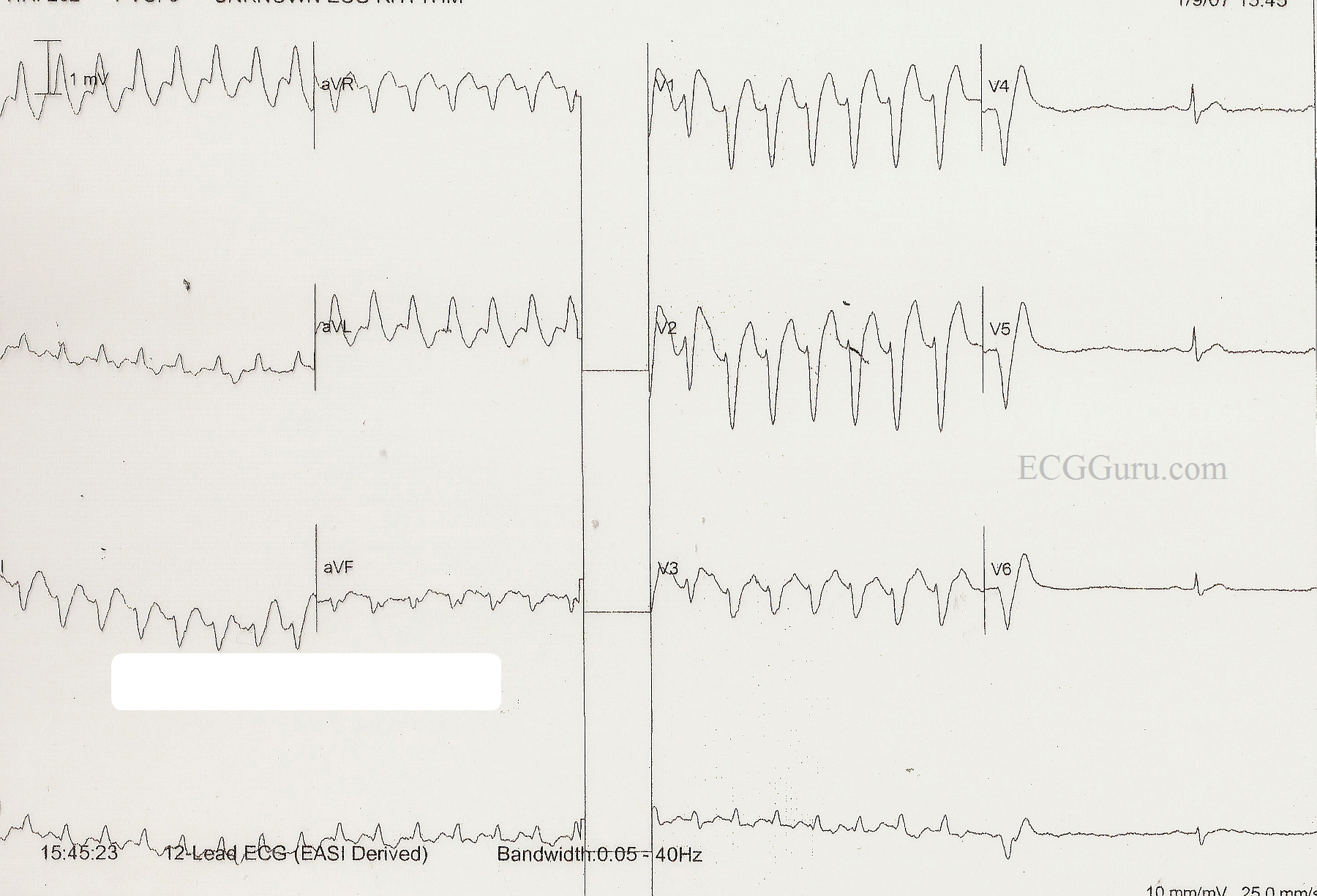
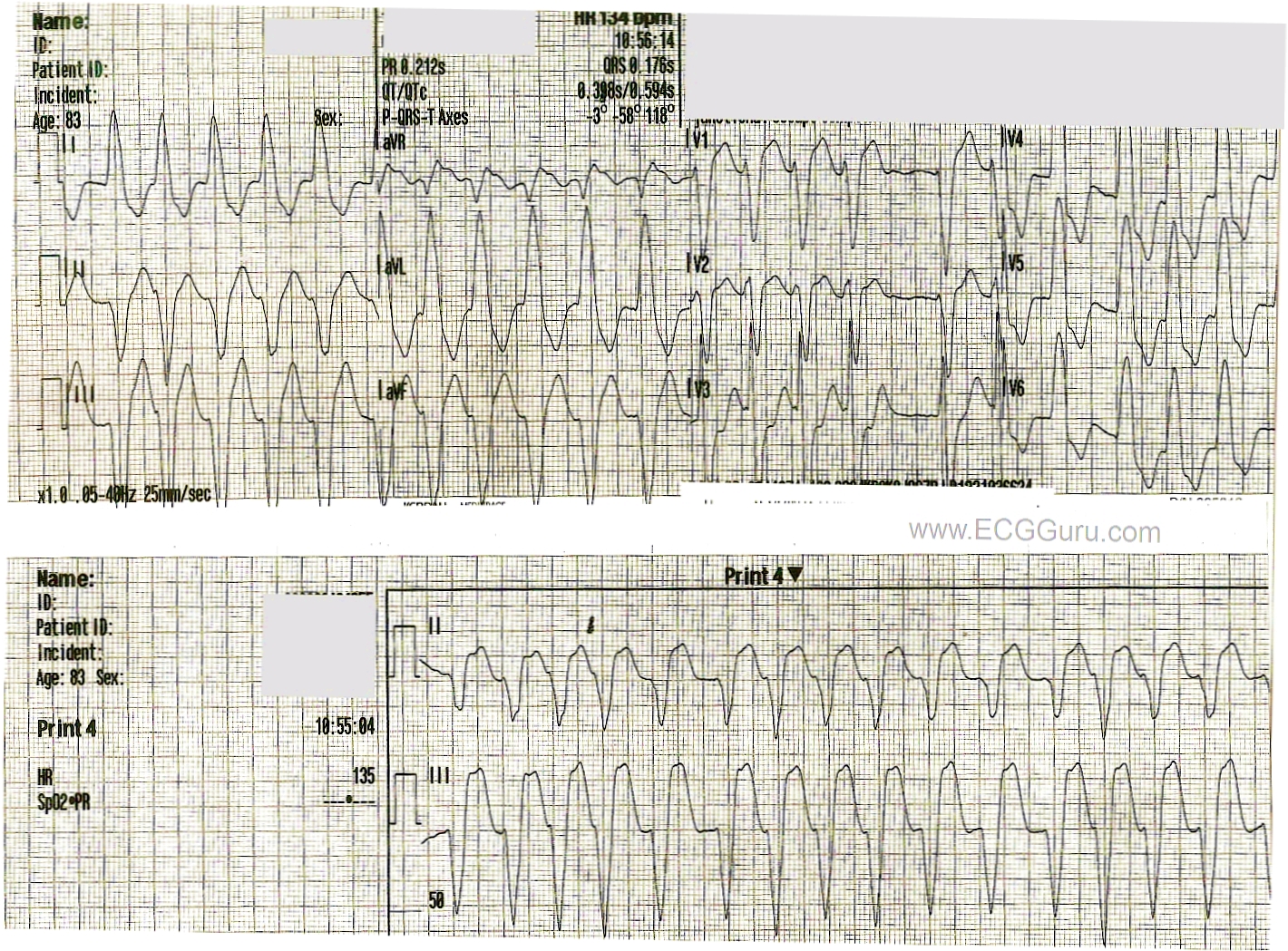
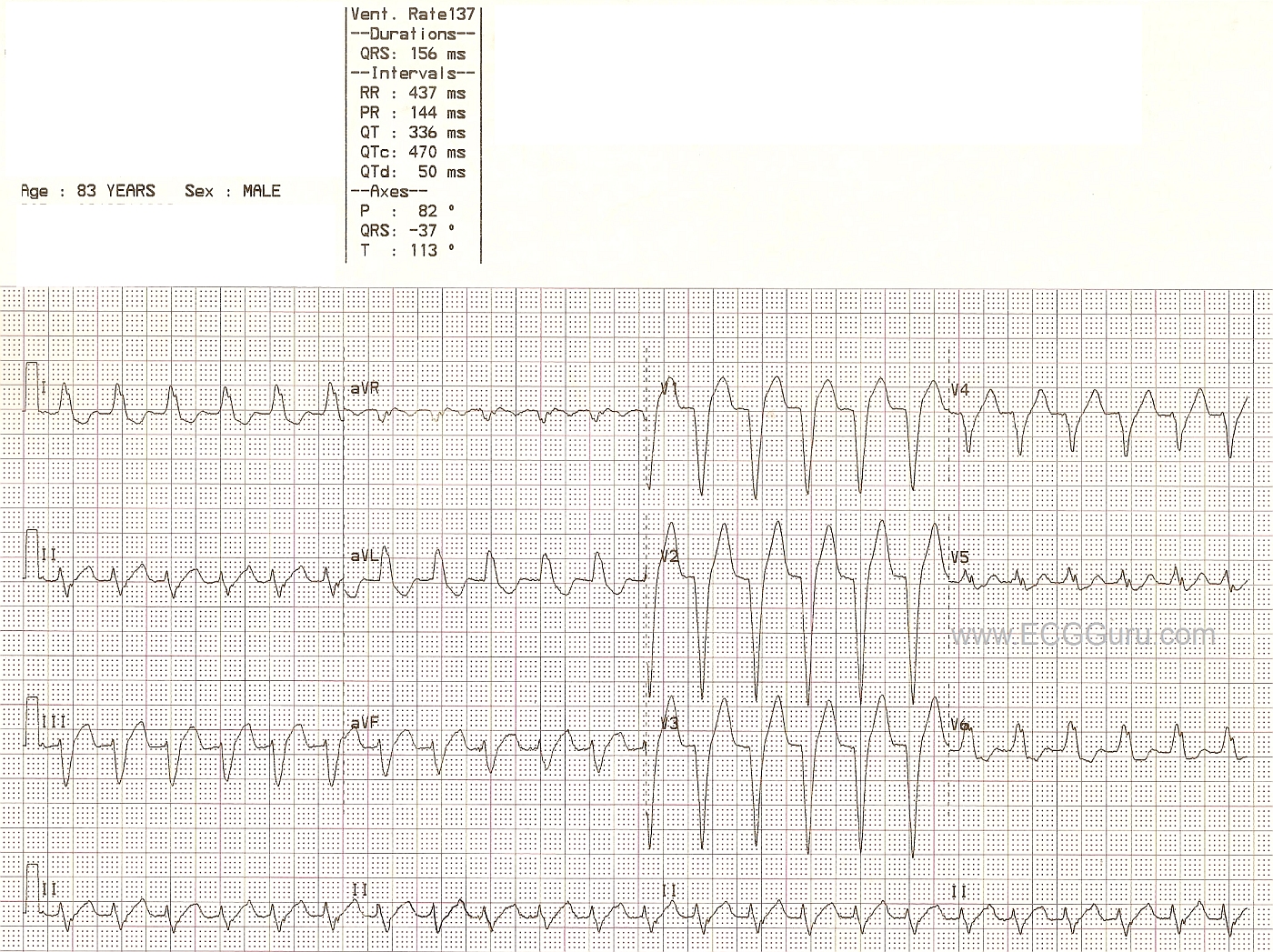
This ECG was presented earlier this week as an example of SVT with LBBB aberrancy, which was ultimately converted with one dose of adenosine in the Emergency Department. It is the most shared and commented on ECG yet to appear on the Guru. The diagnosis given was the one accepted by the medical staff who cared for the patient, who was a man in his 30's who presented to the Emergency Department complaining of a rapid heart rate. He was ambulatory with stable vital signs, in spite of the tachycardia. He reported that he has had several episodes of fast heart rate which responded to either Valsalva maneuvers or, in some cases, medication in the ED. He was told he might benefit from an ablation procedure, but he did not have health insurance and continued to use the ED as his primary source of medical care. When he was admitted to the ED, the tech initially called for help, thinking the monitor showed ventricular tachycardia. The ED physician felt that this represented LBBB aberrancy, possibly rate-dependent, and he treated the patient with adenosine. The rhythm converted to sinus after one dose, and the patient remained stable throughout the process. He was advised to undergo further observation and testing, but he declined due to financial concerns, and the fact that he usually succeeded in relieving his symptoms with "bearing down".
Wide-complex tachycardias can be difficult to assess simply from an ECG. The patient's stability depends more upon general health and cardiac output issues than the origin of the tachycardia. When we presented this ECG, we also presented the diagnosis he had upon discharge from the ED.
Subsequently, ECG Guru Dr. Ken Grauer, a frequent contributer to this site, offered his alternative diagnosis and his explanation of why he believes this to be v tach. Other well-respected ECG experts have also questioned the original diagnosis. Please refer to the comments below for this very helpful explanation. Unfortunately, this patient is lost to followup, as this incident occurred some time ago.
WTCs remain a most fascinating topic, especially for those who enjoy "detective work". We thank Dr. Grauer, Tom Bouthillet, and others for their contributions to the ECG Guru on this topic.